Vibramycin
Vibramycin 100 mg without a prescription
Mullis received because it is quick medicine grapefruit interaction buy vibramycin 100 mg without a prescription, inexpensive and the Nobel Prize and the Japan Prize for simple. To ensure success, care should be taken both in preparing the reaction mixture and setting up the cycling conditions. Increasing the cycle number above ~35 has little positive effect because the plateau occurs when the reagents are depleted; accumulate. This separation allows a quantitative real time polymerase chain more reliable collection and sensitive 14 reaction is a laboratory technique based measurement of nucleic acid amounts. Nested polymerase this is achieved by using various chain reaction is a modification of fluorescent dyes which react with the polymerase chain reaction intended to amplified product and can be measured by reduce the contamination in products due an instrument. It has also long been a standard concept was conceived in 1992 by Sykes method in all laboratories that carry out 13 et al. In this diagnosis of microbial infections and connection the diagnosis of viral diseases epidemiological studies. There are also necessary to detect pathogens outside numerous applications for real-time the body. Clonal have been unpredictable just a halfamplification enabled by single-step century ago. To identify the sites where technique with high sensitivity and they have entered, the known, "internal" specificity. Recent Advances in the Polymerase Comparison of methods for extraction Chain Reaction. Indian Kala-Azar and Assessment of Direct cloning and sequence analysis Cure J Clin Microbiol. Keywords Abstract asthma; children; consensus; guidelines; Asthma is the most common chronic lower respiratory disease in childhood wheeze. Several guidelines and/or consensus documents are availCorrespondence able to support medical decisions on pediatric asthma. Papadopoulos, Department of doubt that the use of common systematic approaches for management can conAllergy, 2nd Pediatric Clinic, University of siderably improve outcomes, dissemination and implementation of these are still Athens, 41, Fidippidou street, Athens 115 major challenges. Accepted for publication 30 May 2012 the principles of pediatric asthma management are generally accepted. To achieve this, patients and their parents should be educated to optimally manage the disease, in collaboration with healthEdited by: Michael Wechsler care professionals. Assessment and monitoring should be performed regularly to re-evaluate and ne-tune treatment. The optimal use of medication can, in most cases, help patients control symptoms and reduce the risk for future morbidity. The management of exacerbations is a major consideration, independent of chronic treatment. There is a trend toward considering phenotype-specic treatment choices; however, this goal has not yet been achieved. Asthma is the most common chronic lower respiratory disIn children, asthma often presents with additional chalease in childhood throughout the world. Asthma most often lenges not all of which are seen in adults, because of the starts early in life and has variable courses and unstable phematuring of the respiratory and immune systems, natural hisnotypes which may progress or remit over time. Wheeze in tory, scarcity of good evidence, difficulty in establishing the preschool children may result from a number of different diagnosis and delivering medications, and a diverse and freconditions; around half of preschool wheezers become quently unpredictable response to treatment. HowIt is therefore not surprising that several guidelines and/or ever, asthma symptoms may persist, often for life, especially consensus documents are available to support medical deciin atopic and more severe cases. These vary in scope and methodolthe quality of life of patients, as well as its cost, is very high. Although there is no doubt that the use major impact on the quality of life of patients and their famiof common systematic approaches for management, such as lies, as well as on public health outcomes (1). Asthma in guidelines or national programs, can considerably improve childhood is strongly associated with allergy, especially in outcomes, dissemination and implementation of these recomdeveloped countries. The criteria used for the formation of can be argued; nevertheless, they are neither necessary for the committee were international representation, relevance to nor exclusive to asthma and therefore do not add appreciably the eld, and previous participation in pediatric asthma to the sensitivity or specicity of the previously mentioned, guidelines. Each member Classications undertook responsibility for preparing tables and relevant commentaries comparing the included documents in a specic To address diversity and guide management, several factors domain. These were subsequently compiled into a rst draft have been used to classify pediatric asthma. In some documents, infantile asthma (<2or pating organizations and submitted for publication. Special characteristics of mendations were extrapolated from the reference documents adolescence are emphasized in most documents. There is slightly less consistency when it comes to severity and persistence, which have been extensively used in the past to classify asthma. Denition With respect to severity, persistent asthma is usually classied the complexity and diversity of asthma in both children and as mild, moderate, and severe. Classications of severity/perproposes a differentiation between pediatric and adult sistence are challenging as they require differentiation between asthma in regard to the denition. Hence, these andtheir patterns, aswellasunderlying mechanisms, at different classications are currently recommended only for initial levelsofdetail. Withonlyminordeviationsintermusage,asthma assessment of the disease severity and are being replaced by the is understood as a chronic disorder, presenting with recurrent concept of control, which is more clinically useful. Slightly different terms are Chronic inammation is recognized as the central patholused for the levels of asthma control, which are generally ogy. In contrast, airway remodeling is only mentioned in the three (controlled, partly controlled, and uncontrolled). Important changes in clinical left) can range from very mild to life-threatening; although not necpresentation take place in relation to age (upper left). Although limessarily discrete, a stepwise approach has been used to characterits are arbitrary and may differ between individuals, infancy, preize severity and inform treatment initiation. More recently, the level school age, school age and adolescence are generally considered of control (lower right) of both current symptoms and risk of future as milestones. Phenotypes (upper right) may result from different morbidity is preferred as a measure, towards which asthma manunderlying pathophysiologies (endotypes), however, there is conagement is evaluated. For many patients, Guideline Update Recommendations several apparent triggers may be identied, also varying over time, highlighting the difficulty in providing a simple phenotype classication system. Levels of control are indicative; the most severe impairment or risk denes the level. Increased populations of mast ment should be addressed in more detail cells, eosinophils, lymphocytes, macrophages, dendritic cells, and others contribute to inammation (25, 26). Structural cells Pathogenesis and pathophysiology such as epithelial cells and smooth muscle cells may also contribute to the inammatory milieu (27, 28). The inammatory There is general agreement that asthma is a disease of and structural cells collectively produce mediators such as chronic inammation, airway hyperresponsiveness, and cytokines, chemokines, and cysteinyl leukotrienes that intenchronic structural changes known as airway remodeling sify the inammatory response and promote airway narrowing. The prevalence of asthma has Acute episodes of airway narrowing are initiated by a comincreased in many countries (12), although in some cases it bination of edema, inltration by inammatory cells, mucus may have leveled off (12, 13). As asthma inception depends hypersecretion, smooth muscle contraction, and epithelial on both genetics (14, 15) and the environment (16), modi desquamation. These changes are largely reversible; however, able environmental factors have been sought in an effort to with disease progression, airway narrowing may become proidentify targets for prevention. Structural changes associated with infections, exposure to microbes, stress, pollutants, allergens, airway remodeling include increased smooth muscle, hyperand tobacco smoke as possible contributing factors.
100mg vibramycin
The major advantage of cromolyn is its safety medications for rheumatoid arthritis vibramycin 100 mg with mastercard, since there are no significant side effects of this drug. In patients with the seasonal type, cromolyn is best initiated just before the season starts at a dose of one spray in each nostril four times daily, and is continued throughout the season. Montelukast (Singulair), a leukotriene receptor antagonist given orally, has a new indication to be used for seasonal allergic rhinitis. Nasal ipratropium (Atrovent), a topical anticholinergic nasal spray, is useful in patients with both allergic and non allergic rhinitis who experience rhinorrhea from various other triggers. It is commonly used as an adjunct therapy if the rhinorrhea symptoms still persist with the antihistamine or intranasal steroid treatment. The decongestants increase nasal patency by inducing vasoconstriction and reducing tissue swelling and obstruction. The decongestants can be useful initially, often coupled with an antihistamine to control active allergic rhinitis symptoms. The side effects of oral decongestants are nervousness, dizziness, tachycardia, shakiness, urinary retention, insomnia. The major concern of nasal decongestants is the prolonged use which may induce rhinitis medicamentosa (especially with topical decongestants), which is rebound mucosal swelling from withdrawal of the medication. Therefore, topical preparations should be used for not more than 3 to 5 consecutive days to prevent rhinitis medicamentosa. Treatment recommendations are as follows: For mild intermittent disease: oral or intranasal H1 antihistamines or intranasal decongestants (for less than 10 days and not to be repeated more than twice a month) or decongestants (not recommended in children less than 12 years old). For moderate-severe intermittent disease: oral or intranasal H1 antihistamines or oral H1-antithistamines or decongestants or intranasal steroids or cromolyn sodium. For mild persistent disease: Same medications as for moderate-severe intermittent above. If the patient has persistent mild symptoms and is on an H1-antihistamine or cromolyn treatment, changing the medication to an intranasal steroid is suggested. The dosage of intranasal steroids may be reduced by half if the patient responds well to the treatment. In seasonal allergy, a shorter course of treatment is required depending on the pollen season. For moderate-severe persistent disease: Intranasal steroids are the first line treatment. If the patient does not improve, consider other reasons for failure to respond to the treatment including heavy persistent allergen exposure. If the major symptom is blockage, doubling the dose of the intranasal steroid is suggested. In the step down treatment, a low dose of intranasal steroid may be required as a maintenance treatment to control symptoms. Referral to a specialist may be considered if the treatment is not fully effective, or if the duration of the treatment is over 3 months and the medications are not helpful. Initial management with allergen avoidance, cold compresses, and lubrication (artificial tears) should be tried before ocular agents are tried. Cold compresses provide considerable symptomatic relief, especially from ocular pruritus and swelling. In fact, all ocular medications provide additional subjective relief when applied immediately after refrigeration. Tear substitutes consisting of saline solution combined with a wetting and viscosity agent, such as methylcellulose or polyvinyl alcohol, can be applied topically 2 to 4 times a day and as needed. However, treatment with oral antihistamines, especially the first generation, may cause eye dryness which interferes with the ocular defense mechanism and increases the potential for ocular irritation and sensitivity. The use of a "topical" agent on the affected eyes is the easiest and most direct therapeutic method. Several topical agents are available for the treatment and the prophylaxis of ocular allergies. These include vasoconstrictors, antihistamines, mast cell stabilizers, and antiinflammatory agents. The combination is more effective than either agent alone or a systemic antihistamine. Topical prescription antihistamines, including levocabastine, emedastine and azelastine, are a good option for symptomatic relief of an ocular allergy. Since these agents do not provide mast cell stabilization, they do not prevent or treat a significant cause of the allergy. Topical mast cell stabilizers include cromolyn, nedocromil, lodoxamide and pemirolast. The relief reported within 15 minutes probably represents a "washout" effect immediately after contact with the eyes. Topical dual action antihistamine and mast cell stabilizers include ketotifen and olopatadine. It inhibits allergen induced prostaglandin production which diminishes the ocular itching and conjunctival hyperemia. Local administration of topical corticosteroids is associated with localized ocular complications such as viral infection, elevated intraocular pressure and cataract formation. Therefore, routine use is not recommended and their use should be under the close supervision of an ophthalmologist. It is also recommended as a treatment for venom or insect hypersensitivity and selected cases of asthmatics. The terms, "allergen vaccination" and "allergen immunotherapy", can be used interchangeably. The dose of specific protein delivered in an allergen extract is crucial for induction of immune tolerance. Adverse effects of allergic rhinoconjunctivitis in children are school absences, poor performance, poor concentration, headaches, malaise, and lethargy as a consequence of sleep disturbance and therefore reduced ability to learn. Furthermore, many of the antihistamines employed have some sedating effects, thereby aggravating the problem. Although genetic factors contribute to the risk of allergic disease development, it is likely that environmental factors are partially responsible for the increase in the prevalence of atopic diseases. Breast feeding for 4-6 months, delaying the introduction of solid food until 6 months of age, and withholding highly allergenic foods such as egg and peanut for 2 to 3 years, especially in a highly allergic family. Reducing exposure to environmental allergens, especially in patients who have already developed respiratory allergies. This hypothesis implies that overcrowding and unhygienic contacts early in life may protect from atopic diseases. The changes of human microbial flora, declining exposure to food-borne and orofecal infections, to helminths and to environmental sources of endotoxin are putative contributors to the rise of allergy cases among populations living with a western lifestyle. Which one is the appropriate medical treatment of an 8 year old girl who develops nasal allergy in spring season The most effective and appropriate for a child with chronic allergic rhinitis and nasal stuffiness is: a. A mother of children with multiple allergic diseases asks you for allergy prevention advice for her next child. His lung examination shows mild wheezing and fair aeration with minimal retractions. The bee sting site on his right forearm is unremarkable with no foreign body seen. He appears to in early anaphylactic shock and he is immediately given subcutaneous epinephrine and an albuterol updraft with improvement of his symptoms. According to one dictionary, it means an exaggerated allergic reaction, while others have defined anaphylaxis as being more severe, involving the respiratory and/or cardiovascular systems. Clinical manifestations include rapid onset of symptoms, a feeling of impending doom, weakness, dizziness, confusion, loss of consciousness and seizures. Airway and pulmonary findings include congestion, sneezing, rhinorrhea, swelling of the lips and tongue, stridor, hoarseness, dyspnea and wheezing. Cardiovascular findings include light headedness, syncope, tachycardia, hypotension, pallor, arrhythmia and complete cardiovascular collapse. Cutaneous findings include erythema, flushing, pruritus, angioedema and urticaria. After the onset of the initial symptoms, symptoms may recur despite initial treatment.
Cheap 100 mg vibramycin with amex
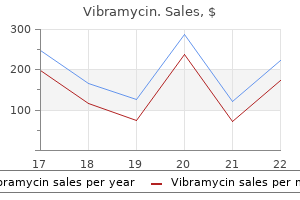
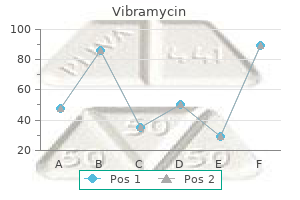
As shown by the linear regression models of assay signals in relation to the Ct values symptoms type 1 diabetes 100mg vibramycin sale, the signal decreases with increasing Ct values. Thus, the assays perform more accurately with samples with more virus and lower Ct values. Moreover, in Honduras, temporary temperature uctuations of stored samples possibly led to protein degradation, aecting sensitivity values. Future studies can expand upon this screen to include more related alphaviruses such as Onyongnyong virus, found in Sub-Saharan Africa, and Ross River virus, found in Australia and the Pacic island regions. Future studies should also aim to analyze assay performance with inactivated serum samples such that point-of-care testing can be used with noninfectious material particularly in areas with limited laboratory capacity. The lateral ow test oers an extremely low-cost and rapid method for early detection in both low and abundant resource settings. Particularly during outbreaks, both assays may enable systems of hospital triage and disease surveillance that better equip public health response. Moreover, an early diagnosis enables more targeted care, avoiding the large costs that hospitals incur from a late diagnosis or misdiagnosis. Early detection of infection can also provide critical data to prevent further transmission and alarm surveillance systems. Ideally, these antigen-based tests may be used in conjunction with serology-based tests, particularly when days of patient fever are uncertain or lie between diagnostic windows. These antigen-based assays are a crucial component to enabling early detection of disease for proper and timely care, economic allocation of clinical resources, and adequate epidemiological measures. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. Chikungunya Virus: Pathophysiology, Mechanism, and Modeling Viruses 1 December 2017. Chikungunya: Epidemiology, Pathogenesis, Clinical Features, Management, and Prevention. Demographic and clinical characteristics of chikungunya patients from six Colombian cities, 2014-2015. Concomitant Transmission of Dengue, Chikungunya, and Zika Viruses in Brazil: Clinical and Epidemiological Findings from Surveillance for Acute Febrile Illness. Viremia and Clinical Presentation in Nicaraguan Patients Infected with Zika Virus, Chikungunya Virus, and Dengue Virus. Dengue and chikungunya among outpatients with acute undierentiated fever in Kinshasa, Democratic Republic of Congo: A cross-sectional study. Simultaneous circulation of arboviruses and other congenital infections in pregnant women in Rio de Janeiro, Brazil. UndetectedChikungunya virus co-infections in a Brazilian region presenting hyper-endemic circulation of Dengue and Zika. Rapid detection and quantication of Chikungunya virus by a one-step reverse transcription polymerase chain reaction real-time assay. Combined detection and genotyping ofChikungunya virus by a specic reverse transcription-polymerase chain reaction. Evaluation of Chikungunya Diagnostic Assays: Dierences in Sensitivity of Serology Assays in Two Independent Outbreaks. Development of an enzyme-linked immunosorbent assay using recombinant protein antigen for the diagnosis of Chikungunya virus. Development of a Highly Protective Combination Monoclonal Antibody Therapy against Chikungunya Virus. Poor Diagnostic Accuracy of Commercial Antibody-Based Assays for the Diagnosis of Acute Chikungunya Infection. Persistent Chronic Inammation and Infection by Chikungunya Arthritogenic Alphavirus in Spite of a Robust Host Immune Response. Detection of Chikungunya Virus Antigen by a Novel Rapid Immunochromatographic Test. Evaluation of an immunochromatography rapid diagnosis kit for detection of chikungunya virus antigen in India, a dengue-endemic country. Diagnostic accuracy of a rapid E1-antigen test for chikungunya virus infection in a reference setting. Historical inability to control Aedes aegypti as a main contributor of fast dispersal of chikungunya outbreaks in Latin America. Fatal cases of Chikungunya virus infection in Colombia: Diagnostic and treatment challenges. Peter Apotheke Volkermarkter Strae 134 9020 Klagenfurt +43 463 311280 ab sofort Karnten Apotheke vorm Lindwurm Neuer Platz 9 9020 Klagenfurt +43 463 512575 ab sofort Karnten Sonnen Apotheke Karawankenplatz 6 9220 Velden am Worthersee +43 4274 2601 ab sofort Karnten Obere Apotheke 10. Aufgrund der starken Nachfrage empfehlen wir Ihnen, vorab telefonisch einen Termin zu vereinbaren, um eine reibungslose Testung zu gewahrleisten. Erhard-Apotheke Petersbrunnstrae 13 5020 Salzburg +43 662 843630 ab sofort Salzburg Wassermann-Apotheke Karolingerstrae 1/Top 2 5020 Salzburg +43 662 82 82 93 ab sofort Salzburg Apotheke zum Lebensbaum Berchtesgadner Str. Lambrecht +43 3585 2280 ab sofort Steiermark Panther-Apotheke Salzburger Strae 255 8950 Stainach +43 3682 222 76 ab sofort Steiermark Apotheke Krems Grazer Vorstadt 152 8570 Voitsberg +43 3142 21202 ab sofort Steiermark Rathaus-Apotheke Hauptplatz 33 8570 Voitsberg +43 3142 225 78 ab sofort Steiermark Apotheke Wies Altenmarkt 31 8551 Wies +43 3465 3611 ab sofort Tirol Pillersee Apotheke Rosenegg 54 6391 Fieberbrunn +43 5354 56450 ab sofort Tirol St. Magdalena Apotheke Unterer Stadtplatz 6060 Hall in Tirol +43 5223 57977 ab sofort Tirol Haller Lend Apotheke Brockenweg 2 6060 Hall in Tirol +43 5223 217 75 ab sofort Tirol Brixental Apotheke Brixentaler Str. Martin Apotheke Eisengasse 25 6850 Dornbirn +43 5572 22384 ab sofort Vorarlberg Lebensquell Apotheke Haselstauderstrasse 29a 6850 Dornbirn +43 5572 201120 ab sofort Vorarlberg Apotheke im Hatlerdorf Hatlerstrae 25 6850 Dornbirn +43 5572 318 09 ab sofort Vorarlberg Stadtapotheke Marktstrae 3 6850 Dornbirn +43 5572 228 52 ab sofort Vorarlberg Sebastian Apotheke Kapfstrae 5 6800 Feldkirch +43 5522 36300 ab sofort Vorarlberg Kreuz-Apotheke Hauptstrae 5 6840 Gotzis +43 5523 53040 ab sofort Vorarlberg Elisabeth-Apotheke Zielstrae 28 6840 Gotzis +43 5523 511600 ab sofort Vorarlberg Rhein-Apotheke Kirchplatz 4 6973 Hochst +43 5578 75391 ab sofort Vorarlberg Rheintal Apotheke Hofsteigstrae 1 6890 Lustenau +43 5577 83344 ab sofort Vorarlberg Engel Apotheke Grindelstrae 17A 6890 Lustenau +43 5577 880800 ab sofort Vorarlberg Kur-Apotheke Schruns Kirchplatz 24/26 6780 Schruns +43 5556 72362 ab sofort Wien Urania-Apotheke Stubenring 2 1010 Wien +43 1 5124463 ab sofort Wien Graben-Apotheke Graben 7 1010 Wien +43 1 5124724 ab sofort Wien Rathaus Apotheke Stadiongasse 10 1010 Wien +43 1 4056678 ab sofort Wien Apotheke "Zum rothen Krebs" Hoher Markt 1 1010 Wien +43 1 533 67 91 ab sofort Wien Apotheke zum Schwan Schottenring 14 1010 Wien +43 1 533 35 41 ab sofort Wien Apotheke fur Dich Engerthstrae 228 1020 Wien +43 1 720 2071 ab sofort Wien Apotheke "Zum guten Hirten" Praterstrae 32 1020 Wien +43 1 2146335 ab sofort Wien Augarten-Apotheke Untere Augartenstrae 13 1020 Wien +43 1 3327562 ab sofort Wien Paulus Apotheke Landstraer Hauptstrae 171 1030 Wien +43 1 7121463 ab sofort Wien Aeskulap Apotheke Kardinal-Nagl-Platz 1 1030 Wien +43 1 7121583 ab sofort Wien Schutzengel-Apotheke Favoritenstrae 11 1040 Wien +43 1 505 01 24 ab sofort Wien Marien-Apotheke Schmalzhofgasse 1 1060 Wien +43 1 5970207 ab sofort Wien Essenz Apotheke Mariahilf Mariahilfer Strae 55 1060 Wien +43 1 586 42 40 ab sofort Wien Apotheke "Zum heiligen Agidius" Gumpendorfer Strae 105 1060 Wien +43 1 596 41 56 ab sofort Wien Walfisch-Apotheke Lerchenfelder Strae 41 1070 Wien +43 1 523 81 79 ab sofort Wien Apotheke zur Kaiserkrone Mariahilfer Str. Sie erhebt keinen Anspruch auf Vollstandigkeit und stellt auch keine Empfehlung der Osterreichischen Apothekerkammer fur die aufgelisteten offentlichen Apotheken dar. Das alleinige Kriterium fur die Aufnahme in die Liste war eine Selbstmeldung der offentlichen Apotheken. Aussagen uber die Qualitat und Validitat der Testergebnisse, die in den offentlichen Apotheken durchgefuhrt werden, sind damit nicht verknupft. Ideal for disinfecting hard, non-porous surfaces as well as sanitizing soft surfaces. Physical Properties Appearance Colorless Fragrance Citrus Form Liquid Formula Ingredients Active Ingredient Ethyl Alcohol 29. Environmental Protection Agency guidelines in effect at the time for determining efficacy of disinfectants intended for use on dry inanimate surfaces. Environmental Protection Agency guidelines in effect at the time for determining acute toxicity of disinfectants intended for use on dry inanimate surfaces. Page 3 of 5 Surface Compatibility Testing Objective Determine product compatibility with common surfaces after extended and repeat contact exposures. Description of Compatibility study to measure the effects of product on the properties of Tests common surfaces. Using a standardized test methodology, many different hard and soft surface materials were exposed to the product under a worst case simulated use condition to simulate approximately one year of extreme use. This product and other commercially available surface disinfectants were soaked for up to 11 cycles in use dilution. Note: Wax or modern polyurethane finishes are not alcohol soluble and do not present incompatibility concerns. Note: Synthetic vinyl fabrics, such as Naugahyde have shown no incompatibility issues during testing. Page 4 of 5 Cleaning Capability Testing Objective Evaluate cleaning performance compared to leading cleaning, sanitizing and disinfecting products found in professional and retail markets. Description of Tests Cleaning Study to measure the effectiveness of soil and organic matter removal from common surfaces. Standardized test methodology used to provide numerical evaluation (0 to 100) of a products capability in removing/cleaning five difficult soils from common surfaces. Data was generated for this product in addition to six leading competitive products. Product Stability Testing Objective Determine if the product meets the performance requirements over the desired two-year product shelf life. Description of Tests Stability Study to measure the properties of product over time (on shelf, unopened, opened). Test Conclusions this product has met the requirements necessary to show that the product is stable for a minimum of two years of shelf life if stored in accordance with label instructions. Because whenever and however you need education content delivered, you can rely on Petersons to provide the information, know-how, and guidance to help you reach your goals.
Buy vibramycin on line amex
There is no specific general symptoms one to four days before rash treatment for Fifth disease treatment goals for anxiety buy vibramycin without prescription. Because transmission of the Fifth disease Although most commonly recognized in children, virus usually occurs before the rash develops anyone is susceptible. Transmission of infection can be lessened by indicate the pregnant women who are exposed to routine hygienic practices for control of Fifth disease and subsequently develop infection respiratory infections, which include hand may have an increased risk for fetal death. Pregnant childcare workers should contact women) should consult their healthcare their obstetricians. The virus that causes Fifth disease has been found in the respiratory secretions of patients and is, therefore, most likely spread by direct person-toperson contact through the respiratory route. Routine exclusion of pregnant women from the workplace where Fifth disease is occurring is not recommended. No, Fifth disease is not reportable by New Hampshire law to the Division of Public Health Services, Bureau of Infectious Disease Control. However, Public Health Professionals are available for consultation at (603) 271-4496. It is very common in in the stool from several days to several months childcare centers; especially those that have after the symptoms have stopped. Treatment is usually necessary for the most common way a person becomes persons with diarrhea. Eating food contaminated How can the spread of this disease be with the parasite may also infect a person. Wash hands thoroughly after using the preparing the food has giardiasis and has some toilet and diapering a child. Staff with stool positive for giardia should drinking water that is contaminated with the not prepare food or feed children. Streams, ponds and springs in New Hampshire are frequently contaminated with Who should be excluded Water can also be Any person with diarrhea shall be excluded from contaminated with giardia when sewage enters the food handling, from childcare agencies and from drinking water supply. There is law to the Division of Public Health Services, usually no fever or vomiting. The diarrhea may Bureau of Infectious Disease Control at (603) last up to several months and can cause significant 271-4496. Spinal fluid is obtained arthritis (an infection and swelling of the joints), by a physician performing a lumbar puncture. Children under Hib, close contacts of this patient age two are most susceptible because their (including family members and persons immune systems are not yet able to fight the having intimate contact such as sleeping bacteria. Rarely, older children and adults may together, hugging and kissing) are at develop infection. However, a carrier may spread be completed at 2 months, 4 months, 6 the bacteria to another person who may then months, and 12-15 months. For unvaccinated children age 15 months or older only 1 dose of the Hib vaccine is required. Children in childcare aged 3-60 months are required to have age appropriate Hib vaccination in order to attend. Parents with specific questions about the Hib vaccine and their child should contact their childs physician. Notify parents or guardians about the occurrence of this illness and urge them to contact their physicians for specific medical care advice. Contact the Bureau of Infectious Disease Control for recommendations about preventing the spread of this illness and assistance in implementing them. Children and staff who are ill with Hib infection should be excluded while they are ill and until 24 hours of antibiotic therapy has been completed. Yes, Haemophilus influenzae infections are reportable by New Hampshire law to the Bureau of Infectious Disease Control at (603) 271-4496. Infected persons who may not seem sick are tongue, inside the cheek and on the gums. The virus may persist in Lesions may also occur on the palms, fingers, the stool for several weeks after the acute illness soles and buttocks. A healthcare provider may diagnose hand, foot and mouth disease based on clinical signs and Who gets this disease The infection is seen primarily in children under 10 years old but may also occur in adults. How can the spread of this disease be Outbreaks of hand, foot and mouth disease among prevented Wash your hands thoroughly after using childcare centers during the summer and early fall the toilet and diapering a child. Wash hands thoroughly after handling respiratory discharges, stool and soiled How is it spread Discourage children from putting toys and secretions of an infected person may spread the other objects in their mouths. Do not allow children to share drinking having contact with infected persons who may not cups or eating utensils. Teach children to sneeze and cough into a infection since the virus may persist in the stool tissue, or into their elbow and away from for several weeks after the acute illness is over. Lesions also occur on the palms, fingers, well enough even if lesions are still soles and buttocks. A low-grade fever may accompany the should be especially careful to adhere to illness for one to two days. People who are going to contract the infection usually do so three to six days after exposure. Hand, foot and mouth disease are not reportable by New Hampshire law to the Division of Public Health Services, Bureau of Infectious Disease Control. In addition, people with hepatitis A are most likely to spread the disease to others during a Who gets this disease Hepatitis A virus is passed out of the body in the There is no treatment that cures hepatitis A. Contact with stoolprevent illness in people exposed to patients with contaminated food, drink or environment surfaces hepatitis A. Wash hands thoroughly after diapering setting because most young children with hepatitis children. Wash hands thoroughly before preparing without symptoms who are in diapers could easily food. Discourage children from putting nonfood items into their mouths since these items may be a source of the virus. Persons with hepatitis A (or suspected hepatitis A) should be excluded from daycare centers, food-handling occupations, and direct care of hospitalized and institutionalized patients for one week after the onset of symptoms (jaundice) or hepatitis A has been ruled out. A Public Health Professional will advise individuals regarding specific recommendations. Yes, hepatitis A is reportable by New Hampshire law to the Division of Public Health Services, Bureau of Infectious Disease Control at (603) 271-4496. It is important that cases associated with a childcare center be reported as soon as possible. A Public Health Professional will give specific recommendations for immunization of the people exposed. Only blood, semen, vaginal fluids and saliva have (Please see Immunization requirements page been shown to be infectious. Standard precautions should be in effect at infected person into the open skin or the eye, nose all times. Disposable gloves should be used or mouth of another person), or through sexual when dealing with any bodily fluids contact. Note: salivary transmission has rarely (blood/body fluid-soiled items, surfaces or occurred and generally through bites.
Diseases
- Chromosome 14, trisomy mosaic
- Xk aprosencephaly
- Pulmonary cystic lymphangiectasis
- Eosinophilic cryptitis
- Polydactyly cleft lip palate psychomotor retardation
- Acrodysplasia
- Boucher Neuhauser syndrome
- Spinal atrophy ophthalmoplegia pyramidal syndrome
- Alexander disease
Cheap 100mg vibramycin with mastercard
On right or leftsided spasm at the onset of epileptic paroxdistributed neuronal networks could presumably be elicited ysms 714x treatment 100 mg vibramycin with visa, and on crude sensation warnings, and elaborate states. Commission on Classification and Terminology of the International temporal isocortex and various limbic structures. Proposal for revised clinical and electroencephaloForced thinking refers to an awareness of intrusive stereographic classification of epileptic seizures. Occipitotemporal epilepsy studied with stereotaxically implanted depth electrodes and successfully treated by temporal resection. The temporal sequence of aura-sensations in patients with complex focal seizures with particular attention to ictal aphasia. There is no consensus on the range of phenomena to be Complex Partial Seizures and Their Treatment. Mental phenomena evoked by an autonomic aura by some, although there is insufficient evielectrical stimulation of the human hippocampal formation and amygdala. Correlative study of interictal electroencephalogram and aura in complex partial seizures. Complex partial seizures: clinical sensations as not being able to breathe, a need to breathe more characteristics and differential diagnosis. Semiology of temporal lobe seizures: value in deeply, and of a breath filling the chest that would not expire. An examination or persistent auras in surgically supplementary sensorimotor area: results of extraoperative electrical stimtreated epilepsy. Relationship of hallucinations to surgery: the impact of measuring health-related quality of life. An uncommon manifestation with localizamygdaloid stimulation in man by interview content and context. The role of the limbic system in expelobe bearing on the localization of the sense of smell and on the interpretariential phenomena of temporal lobe epilepsy. The anatomy of epileptic auras: focal induced on stimulation by subdural electrodes. The localizing value of auras in partial seizures: a occurring in epilepsy produced by depth stimulation. Longitudinal clinicoelectrophysiorecorded with surface and depth electrodes in patients with temporal lobe logic study of a case of Lafora disease proven by skin biopsy. Autonomic auras: left hemispheric preand motor areas of human cerebral cortex as determined by direct recorddominance of epileptic generators of cold shivers and goose bumps New York: predominate in women with temporal lobe epilepsy: a finding suggesting Macmillan; 1950. Orgasmic aura originates from the right ical and electroencephalographic findings. These two concepts are intiseizures arising from the mesial temporal lobe with an aura of mately related, but it is important to recognize that they are deja vu, staring, unresponsiveness, and stereotyped oroaliessentially distinct: while consciousness as a whole is clearly mentary and hand automatisms. These issues lead to the impaired in epilepsy patients who are completely unresponproposition of a five-tier classification system that distinsive during their spells, and are later amnestic of their events, guishes the seizure characteristics (including semiological the question is a bit more controversial in other cases. In this semiological classification, a seizure is defined solely occurred during the seizure (2). A dialeptic (from the may not obey any commands during a seizure, but do recall Greek word dialeptin meaning to stand still, to interrupt, when interviewed postictally all the commands and instrucor to pass out) seizure is one with impairment of conscioustions given during the ictus. An automotor seizure possible scenarios including ictal aphasia, inability to perform would be one with predominant automatisms regardless of voluntary movements secondary to stimulation of negative whether consciousness was impaired or not. In this chapter, we motor areas, or diversion of attention by a hallucinated expewill use the general term of complex partial seizures, as well as rience (3). These examples illustrate the conceptual complexthe more specific terms of dialeptic and automotor seizures ity of assessing consciousness in relation to epileptic seizures when a distinction between the two is needed. Recently, entiation of focal from generalized seizures causing an impairsome epilepsy centers have even proposed the use of a stanment of awareness. Then, we will focus on characterizing the dardized Consciousness Inventory to assess the level and localizing value of focal seizures with impaired consciousness, content of ictal consciousness (4,5). For the purposes of this and discuss lateralizing features that may help in further definchapter, we will use the term focal epilepsy with impaired ing the epileptogenic focus. We then describe typical electroenconsciousness to refer to focal epilepsies where either cephalographic findings and conclude with a section on the responsiveness or awareness/recall is disturbed during the ictal proposed mechanisms of impaired consciousness in partial period. The terms it possible to identify the characteristic interictal and ictal feacomplex partial and absence refer therefore to electroclinical tures of these seizures. Furthermore, the broad Gibbs, and Lennox also noted interictal sharp waves in the temumbrella of complex partial seizures encompasses various poral regions in patients with this seizure type. So, a clear distinction than its actual pattern, and that this pattern originated from between dialeptic seizures seen in the setting of frontal or temdeep within the temporal lobes, near the midline (11). The Paris group (16) published a number of understanding of the symptomatology of focal seizures with papers on frontal lobe epilepsy. Tharp (17) was the first to impairment of consciousness arising from various locations identify seizures with loss of consciousness arising from the (22,28). Some studies Escueta and colleagues described three types of complex employed cine film and analyzed photographs taken at three partial seizures (23). The introduction of videotape technology proseizures) begins with a motionless stare or behavioral arrest vided an inexpensive and effective way to easily record and (phase 1) quickly followed by a period of unresponsiveness play back seizures as often as needed, resulting in a better grasp and stereotyped automatisms (phase 2) evolving to a final of phenomenology. The observations of Delgado-Escueta, phase of a clouded state and semipurposeful reactive Theodore, Williamson, Quesney, Bancaud, and others vastly automatisms. The localizing value of the Psychomotor Seizure, Wieser (26) described the order of motionless stare was believed to indicate mesial temporal lobe symptom onsets and symptom clusters, and attempted to corepilepsy (23). However, behavioral arrest is also seen in 20% relate these clusters with electrographic activity recorded of patients with frontal lobe epilepsy (31). Using methods similar to those of Wieser, Kotagal depending on the location of the ictal seizure pattern. Frontal examined temporal lobe psychomotor seizures in patients lobe seizures are more likely to manifest with loss of orientawho were seizure-free after temporal lobectomy (28). Similar tion behavior and expressive speech; left temporal lobe methods also have been used to study frontal lobe seizures seizures lead to impairments of memory and expressive and (29,30). The auras last from a few seconds to common focal type after temporal lobe seizures (20). Seizures with loss of consciousrecovery later in the seizure may allow the patient to look at ness can arise from various locations within the frontal lobe an observer walking into the room or interact in some other (except from the rolandic strip) (17,29,30,34). Bizarre than 10 seconds, which helps to distinguish them clinically attacks with prominent motor automatisms involving the from typical absence seizures characterized by 3-Hz spikelower extremities (pedaling or bicycling movements), sexual wave complexes (23). Identification of seizure onset within the frontal Chapter 12: Focal Seizures with Impaired Consciousness 155 lobe by semiology alone and differentiation of mesial temporal in approximately 60% of temporal lobe seizures (28). Attempts to restrain them may only aggraconvexity, tonic seizures from the supplementary motor area, vate matters. Violence, invariably nondirected, may be seen and automotor seizures from the orbitofrontal region (35). The patient is usually amnestic for the Seizures with motor agitation and hypermotor features are seizure but may be able to recall the aura. A few patients may more likely to arise from the orbitofrontal and frontopolar exhibit retrograde amnesia for several minutes before the regions, as opposed to seizures with oroalimentary automaseizure. Up to 50% of are characterized predominantly by behavioral arrest with patients develop complex partial status epilepticus (35). In younger limbs that is often bilateral but may be asymmetric and is children, symmetric motor phenomena of the limbs, postures accompanied by nonpurposeful movements of uninvolved similar to frontal lobe seizures in adults, and head nodding as limbs and vocalizations. Because of their bizarre symptomato test for consciousness in infants, focal seizures with impairtology, they are sometimes mistaken for nonepileptic seizures. In very young infants, these may also occasionCingulate gyrus seizures may also vary in semiology. Seizures arising from the anterior portion of the cingulate present with predominantly motor manifestations such as bilateral asymmetric tonic seizures, hypermotor seizures, and Seizures of Parietal Lobe Origin complex motor seizures, while posterior cingulate cortex epilepsies tend to predominantly have alterations of conLike seizures of occipital lobe onset, partial seizures from the sciousness (dialeptic seizures) and automatisms of the distal parietal lobe may manifest loss of consciousness and automaportions of the limbs (automotor seizures) as the main clinical tisms when they spread to involve the temporal lobe. The vocalizations may consist of unintelligible function may occur in seizures arising from the dominant screaming or loud expletives of words or short sentences. Also described in parietal lobe complex partial Patients also may get up and run around the room. In a study of 40 patients with parietal lobe as dizziness, epigastric sensation, or fear in 50% of patients; epilepsy as established by standard presurgical evaluation, behavioral arrest in 20%; and speech arrest in 30%.
Purchase vibramycin from india
Recommends children with warts should to avoid use of ffteen-passenger vans and use vehicles not be excluded unless meet certain criteria medicine of the future buy cheap vibramycin 100mg online. Outlines process rent Centers for Disease Control and Preventions Recomfor inclusion/exclusion of children or staff with lymphadenimended immunization schedules for persons aged 0 through tis. Note: Infectious Diseases was formerly Chapter immunized should be excluded immediately if there are 6 in the 2nd Ed. Recommends not excluddocumentation that a child six months of age and older has ing children and staff unless meet certain criteria. Lesions current annual vaccination against infuenza unless there should be covered. Overall: Improved consistency of language, referring to children with special health care needs. Recommends contents of a plan in the areas of planning and coordination, infection control Standard 10. Includes advice for both foster parents and caregivers/teachers on how to make successful transitions for children into an early care and education program. Supervision is recommended the small family child care home caregivers/teachers own for toddlers and preschoolers to ensure safety and prevent children as well as any other children in the home temporarbehaviors such as inappropriate touching or hurting other ily requiring supervision should be included in the child:staff sleeping children from taking place. Some states are setting limits on the number ratio allow threeto fve-year-old children to have continuing of school-age children that are allowed to be cared for in adult support and guidance while encouraging independent, small family child care homes. In child care, these children do not come from the same family and must learn a set of common rules that may differ Unscheduled inspections encourage compliance with this from expectations in their own homes (6,8). Effects of child-caregiver ratio on the interactions between 9to 12-year12:1 24 caregivers and children in child-care centers: An experimental olds study. Children over thirty-one months of age can Services, Offce of the Assistant Secretary for Planning and usually be organized to nap on a schedule, but infants and Evaluation. New York: Cambridge University child should be moved to another activity where appropriate Press. Ratio Children with special health care needs or who require more 12 months 2:1 6 attention due to certain disabilities may require additional staff on-site, depending on their special needs and the ex13-23 months 2:1 8 tent of their disabilities (1). Howevbreaks, and staff training, one staff person should stay in the er, larger groups are generally associated with less positive nap room, and the above staff activities should take place interactions and developmental outcomes. Group size and in an area next to the nap room so other staff can assist if ratio of children to adults are limited to allow for one to one emergency evacuation becomes necessary. If a child with a interaction, intimate knowledge of individual children, and potentially life-threatening special health care need is presconsistent caregiving (7). Caregivers/teachers must be recognized as performing a Group size is the number of children assigned to a carejob for groups of children that parents/guardians of twins, giver/teacher or team of caregivers/teachers occupying an triplets, or quadruplets would rarely be left to handle alone. Each state has its caregiver/teacher, and may result in loss of the caregivers/ own set of regulations that specify child:staff ratios. The Care and Development Block Grant: Improving quality child care for facility may wish to increase the number of staff members if infants and toddlers. Early childhood program standards and Child:staff ratios established for out-of-home child care accreditation criteria. Fatalities and the organization of to focus entirely on driving tasks, leaving the supervision child care in the United States. Serving Children with Special Health Care In any vehicle making multiple stops to pick up or drop off Needs and Disabilities children, this also permits one adult to get one child out and take that child to a home, while the other adult supervises Facilities enrolling children with special health care needs the children remaining in the vehicle, who would otherwise and disabilities should determine, by an individual assessbe unattended for that time (1). The facility should have care have occurred when children were mistakenly left in suffcient direct care professional staff to provide the vehicles, thinking the vehicle was empty. Policy statement: Prevention of should remain in direct physical contact with an infant at all drowning. Pool and thirteen months and up to fve years of age are in or around spa safety: the Virginia Graeme Baker pool and spa safety act. Consumer Product staffng requirements and environmental modifcations may Safety Commission. American Academy of Pediatrics, Committee on Injury, Violence, self-locking gates around all swimming pools, hot tubs, and Poison Prevention, J. Although Switzerland ranked twenty-frst with these shifts in central nervous system structure and funcfourteen versus twenty-four weeks as compared to the U. At approximately eight to twelve weeks after ternity leave for qualifying employees (16,20). On-the-job moms: Work and breastfeeding initiation and duration for a sample of low-income women. New York: tries including Australia, New Zealand, Canada, United Allyn and Bacon Classics. Chapter 1: Staffng 8 Caring for Our Children: National Health and Safety Performance Standards Pediatric Clinics North Am 53:167. Maternity leave in the b) Accommodation is unreasonable or will result in United States: Paid parental leave is still not standard, even among undue hardship to the program; the best U. Commonly asked questions about child care centers health, children should be protected from any risk of abuse and the Americans with Disabilities Act. Having a Directors of centers and caregivers/teachers in large and state credentialing system can reduce the time required to small family child care homes should conduct a complete ensure all those caring for children have had the required background screening before employing any staff member background screening review. The background ground screening record should contact their state child screening should include: care licensing agency for the appropriate documentation a) Name and address verifcation; required. Court c) Education verifcation; records are public information and can be obtained from d) Employment history; county court offces and some states have statewide online e) Alias search; court records. When checking for prior arrests or previous f) Driving history through state Department of Motor court actions, the facility should check for misdemeanors Vehicles records; as well as felonies. Driving records are available from the g) Background screening of: State Department of Motor Vehicles. The National Association of family child care homes should also have background Professional Background Screeners. Failure of the prospective employee to disclose previous history of child abuse/neglect or child sexual abuse is grounds for immediate dismissal. Past experience working in an early b) A valid certifcate of successful completion of childhood setting is essential to running a facility. The exact comg) Oral and written communication skills; bination of college coursework and supervised experience is h) Certifcate of satisfactory completion of instruction in still being developed. Cost, quality and child outcomes in child effect on quality child care, whereas experience per se has care centers. Standards for early childhood professional the director of a center plays a pivotal role in ensuring the preparation programs. National Association for the Education of Young Children may employ a director who teaches as well. Worthy work, al substitute teaching may keep the director in touch with unlivable wages: the national child care staffng study, 1988-1997. At least 50% of all assistant teachThose teachers with a four-year college degree exhibit optiers and teacher aides must have or be working on either a mal teacher behavior and positive effects on children (6). For additional information on qualifcations volunteers should never be left alone with children. Standards for Early Childhood professional health professional, or an early childhood mental health conpreparation programs. Young Children allowed to pursue their interests within safe limits and to be (September): 1-7. From neurons to Development neighborhoods: the science of early childhood development. Services, Offce of the Assistant Secretary for Planning and Balancing free exploration with organized activities includEvaluation. Supment, and safety of individual children, children as a group, port from a mental health professional may be needed. Local concerns, including health-related parent/guardian/staff mental health agencies or pediatric departments of medical observations, health-related information, and the provision schools may offer help from child psychiatrists, psycholoof resources. An internal advocate for issues related to of children who need further medical assessment or health and safety can help integrate these concerns with updating of their information; other factors involved in formulating facility plans.
Cheap vibramycin 100mg
Early administration of Aspirin has been shown to decrease mortality in Acute Coronary Syndrome symptoms pulmonary embolism buy vibramycin 100 mg without a prescription. In the un-intubated patient, analgesics may not be administered in combination with benzodiazepines without Direct Medical Oversight. Consider administration of one of the following prior to/during pacing, if feasible: o Midazolam 0. For symptomatic beta blocker or calcium channel blocker overdose, consider glucagon 0. After 4 cycles (8 minutes): o Continue 2 minute cycles of uninterrupted chest compressions. Consider termination of efforts or not attempting resuscitation (see Do Not Resuscitate Orders 6. After 4 cycles (8 minutes): o Consider endotracheal intubation or use of an alternative airway without interrupting chest compressions. Minimize interruptions in chest compression, as pauses rapidly return the blood pressure to zero and stop perfusion to the heart and brain. Mechanical devices should only be used by services that are practiced and skilled at their application. Perform chest compressions while defibrillator is charging and resume compressions immediately after the shock is delivered. Protocol Continued If feasible and the scene is safe, immediately upon arrival, one member of the crew should rapidly enter the scene without equipment (other than gloves) to begin chest compressions. Move furniture or get the patient in a position that will allow a rescuer space to kneel on both sides of them, and where there is sufficient room at the head. Therefore resuscitate the patient as close to the scene as operationally feasible. Position 1 and 2 are ideally set up on opposite sides of patients chest and perform continuous chest compressions, alternating after minute to avoid fatigue. Ventilate 1 breath every 10 compressions during recoil without interrupting chest compressions. With the goal of immediate uninterrupted chest compressions, if a mechanical device is used, it should not lead to delay or interruption in chest compressions; consider delayed applications. Pre-charge manual defibrillators prior to rhythm check to ensure rapid defibrillation if a shockable rhythm is present. Consider treatable causes: hypoxia, overdose/poisoning, hypoglycemia, hypothermia, and hypovolemia (treat as per specific protocol). If Return of Spontaneous Circulation occurs see Post Resuscitative Care Protocol 3. Placement of an advanced airway during cardiac arrest should not interrupt chest compressions. Avoid nitroglycerin in any patient who has used a phosphodiesterase inhibitor such as: sildenafil (Viagra, Revatio), vardenafil (Levitra, Staxyn), tadalafil (Cialis, Adcirca) which are used for erectile dysfunction and pulmonary hypertension. Allow the patient to be in their position of comfort to maximize their breathing effort. Avoid hyperventilation as it increases intrathoracic pressures, potentially worsening hemodynamic instability. If symptomatic and hemodynamically unstable: Synchronized cardioversion: Follow manufacturers recommendations for dosing. Consider administer of one of the following prior to or during cardioversion, if feasible: o Midazolam 2. If symptomatic, but hemodynamically stable: For narrow complex tachycardia (with a heart rate persistently >150bpm): Attempt vagal maneuvers, for regular rhythms. Medications should be administered cautiously in frail or debilitated patients; lower doses should be considered. Wide complex tachycardia should be considered Ventricular Tachycardia until proven otherwise Signs and symptoms of hemodynamic instability: o Hypotension o Acutely altered mental status o Signs of shock o Signs of acute heart failure o Ischemic chest pain Adenosine should be administered rapidly though a proximal. If adenosine is ineffective or for wide complex, perform synchronized cardioversion: o 1 J/kg; if unsuccessful, increase to 2 J/kg. Consider administration of one of the following prior to or during cardioversion, if feasible: o Midazolam 0. Assess the patients airway for evidence of smoke inhalation or burns: soot around mouth or nostrils, singed hair, carbonaceous sputum, see Smoke Inhalation Protocol 2. If a partial thickness burn (2nd degree) is <10% body surface area, apply roomtemperature water or room-temperature wet towels to the burned area for a maximum of 15 minutes. For suspected or verified Hydrofluoric Acid skin exposure: a) Apply gauze soaked with 2. Consider spinal motion restriction for electrical burns that result in hand to hand flow. If a partial thickness burn (2nd degree) is <10% body surface area, apply room-temperature water or room-temperature wet towels to the burned area for a maximum of 15 minutes. Patients who sustain an electrical burn should be placed on a cardiac monitor Consider spinal motion restriction for electrical burns that result in hand to hand flow. Consider spinal motion restriction for suspected spinal injury, see Spinal Trauma Protocol 4. Conscious patients with submersion injuries should be transported to the hospital. Chemical irritants, including pepper spray: flush with copious amounts of water, or normal saline. If the patient cannot close their eyelids, keep their eye moist with a sterile saline dressing. Dental avulsions should be placed in an obviously labeled container with saline soaked dressing, milk, or cell-culture medium (example: Save-a-tooth). Avoid touching the root of the tooth (the part of the tooth that was embedded in the gum) because it can be damaged easily. Remove obvious debris, irrigate open wounds with saline solution, and cover with moist sterile dressing. Assess Circulation-Sensory-Motor distal to injury before and frequently after immobilization. Stabilize suspected pelvic fractures in the presence of hypotension or other signs of shock with an appropriate commercial device (preferred) or bed sheet. Paramedics may straighten severely angulated fractures if the distal extremity has signs of decreased perfusion. Paramedics may contact Direct Medical Oversight for any other reductions not meeting this protocol. For dislocations due to direct impact, such as falls, the injury is more likely to be complicated by a fracture. Fractures of the humerus, pelvis and femur, as well as fractures or dislocations involving circulatory or neurological deficits, take priority over other musculoskeletal injuries. Hip dislocations, pelvic, knee, and elbow fracture / dislocations have a high incidence of vascular compromise. Neurogenic shock: May occur after an injury to the spinal cord disrupts sympathetic outflow resulting in unopposed vagal tone. Control active bleeding using direct pressure, pressure bandages, tourniquets (commercial preferred) see Tourniquet Procedure 6. Do not delay transport; consider hospital destination per Trauma Triage and Transport Decision Protocol 6. Total volume should not exceed 2000 mL without consultation with Direct Medical Oversight. If cardiac tamponade is suspected, rapid transport and treat arrhythmias per Cardiac Protocols 3. Hemostatic bandages must be non-exothermic type that washes off with normal saline. Delaying aggressive fluid resuscitation until operative intervention may improve outcome. Patients should be reassessed frequently, with special attention given to the lung examination to ensure volume overload does not occur. Patients without any of the above findings should generally be transported without the use of a cervical collar or other means to restrict spinal motion.
Generic 100mg vibramycin amex
Access and availability of pediatric subspecialty services must not be significantly impeded by managed care arrangements medicine game buy generic vibramycin on line. A good pediatric primary care physician should also work with non-physician partners. Interactions with school personnel, public health nurses, social workers, various therapists (such as speech/language therapists, occupational therapists, physical therapists), early Page 18 childhood educators or daycare providers are a common part of pediatric practice today. Learning to interact appropriately with these individuals, and to gain from their expertise, is an important part of pediatric training. True/False: When caring for pediatric patients, it is always more appropriate to use pediatric subspecialists than specialists who may be primarily trained to work with adults. True/False: There is a standard for after hours accessibility that all pediatricians adhere to . True/False: There is variability in the use of pediatric subspecialty care that results from factors other than availability of specialists. If a pediatric subspecialist is not available, the pediatrician has the following choices: a. Many factors are involved, including the training of the primary care pediatrician and past experience with similar cases. She is now being breast-fed once a day, given pumped breast milk in a bottle two to three times a day, and formula the rest of the time (about 16 oz or 480 ml per day). The monitoring of a childs growth is probably the most important job for a pediatrician. It is not only essential for the general pediatrician, but for other subspecialties as well. An aberration in growth patterns is often the first clue that there is something wrong with the child. Often, the growth of the child is used in conjunction with other signs and symptoms, to help the physician determine what the problem might be. An older child who is not gaining weight could be the first clue to inflammatory bowel disease. The most important tool for assessing and monitoring a childs growth is the growth chart which plots height (length), weight and head circumference. The larger, pooled data sets used to create the revised charts eliminate the problem of differing percentiles when making the transition from recumbent length to stature height. Other new features of the new growth charts are the extension to 20 years because of sufficient data being available and its desirability for general populations, particularly for clinics dealing with endocrine disorders and congenital abnormalities (1). There are other growth charts available for children with various conditions, such as Turner, Klinefelter and Down syndromes and achondroplasia (2). Special growth charts for premature babies are also available by Babson and Benda that are based on gestational rather than chronological age, beginning at 26 weeks of gestation (3). Size at age 2 years correlates with mean parental height, reflecting the influence of genes. A formula can be used to calculate the estimated adult height by taking the mid-parental height (mothers height + fathers height, divided by 2), and adding 6. In adolescents, normal variations in the timing of the growth spurt can lead to a misdiagnosis of growth abnormalities. In primary care, it is important to know the relationship between sexual maturity and growth, which is beyond the scope of this chapter. This is also around the time when the nipple and areola have developed but before any other significant breast development (7), and about 6 to 12 months prior to menarche. After menarche, females will usually not grow more than 5 cm, with epiphyseal closure occurring about 2 years after. The periods of rapid growth occur during the first 12 months of age, and from puberty until adulthood. Calculation of weight gain in grams per day also allows more precise estimation of growth rate as can be seen in the table below. Page 20 Approximate Approximate Age Daily Weight Gain Monthly Weight Gain 0-3 mos 30 g 1 kg (2 lb) 3-6 mos 20 g 0. When curves are outside the 5th and 95th percentiles, it is useful to mention the age at which the growth parameter is at its median value (50th percentile). For example, if a 10 year old female weighs 18 kg, this weight is below the 5th percentile for a 10 year old; and, it is at the 50th percentile for a 5 year old. The problem with the weight for height curves is that they are applicable only from 2 years to 11. However, since the cutoff values for children differ with age and sex, they therefore must be based on percentiles, with the 85th percentile being suggested as the cutoff point for being overweight. Fat-free mass increases with age in both sexes, but increases are more rapid in boys than in girls after age 13. The growth curve has the following appearance: weight and height drop in their percentiles near the end of infancy, parallel the norm through middle childhood, and accelerate toward the end of adolescence. Adult size is normal or often taller than average because their duration of growth is longer than others. At what age does the uterine environment play a role in the growth of a child versus the influence on growth by the genetic makeup What is the formula used to estimate a childs adult height (Tanners height prediction formula) The physicians in the clinic are mandated to do a check of development but they do this somewhat differently from physician to physician. Another physician asks questions to her parents but does not use any formal developmental screening instrument. On further questioning the childs family relates how she likes to play by herself, and is easy to care for as she doesnt need too much attention. Later at three years of age, the parents are very worried about the childs language but are told that many children are "late talkers". The parents become angry as they find that many characteristics they have seen in the past two to three years are noted by the school psychologist as signs of autism. They tell the psychologist that they feel that their physician should have figured this out earlier. An important aspect of caring for children in a medical context is that they grow in multiple ways over time. Developmental or behavioral conditions are thought to occur in 12 to 16% of children in the United States (1). Physicians such as pediatricians and family practitioners have essential roles because of their frequent contact with children and their families. They have knowledge of normal and abnormal development unlike other professionals who are in touch with families. Directly observed developmental behavior may be different than when the child is well (3). Families also have more trust with someone who gets to know their child and family well. Obvious and severe problems are actually rare compared to more commonly seen but subtle problems. Informal "eyeballing" of children and informal questioning of parents do not work well. There is a good chance of missing problems because of the need of looking at multiple domains in development. Research from Great Britain where clinical impression is used rather than screening tests is revealing. These tools should be used on whole populations of children as to not miss children with subtle (and sometimes not so subtle) problems. Goals of early management include optimizing the childs development, and supporting families with these children well. However, most of the items require direct observation of the child trying to do certain tasks. It has several advantages including ease of administration, coverage of a good range of age groups to screen (from birth to about 6 years of age), and a normative sample that includes diversification of race, place of residence (urban, suburban, rural) and the mothers educational level (7). One type of screening that is growing in popularity, and bolstered by recent research findings is a standardized parent questionnaire. Concerns about the accuracy and bias of parent reporting, parent reading level, and their understanding of concepts regarding the standardized parent screening tools have not been shown to be major problems after research has been done regarding these tools. The interpretation also helps guide the clinician in whether to use a hands-on screening tool, give parental reassurance, monitor the child, or make specific referrals to other specialists (6). Because development is ongoing with time, and because measuring development at very young ages cannot evaluate the full complexity of the various developmental domains at later ages, it is important to continue to assess children using tools appropriate for their age throughout their entire development.