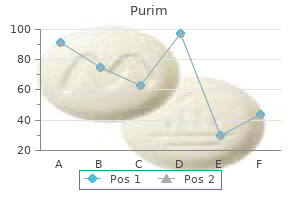
Purim
Buy purim us
Early defibrillation of V-Fib or pulseless V-Tach is closely correlated with neurologically intact survival symptoms 10 days post ovulation order 60caps purim free shipping. The most important goal in the treatment of sudden cardiac death is to provide diagnosis and electrical defibrillation of V-Fib/pulseless V-Tach as soon as possible after onset. Do a rapid scene survey/tactical assessment to determine any threats in the immediate area. If the patient is not breathing, give rescue breaths that cause the chest to rise. Determine cardiac rhythm and initiate the appropriate resuscitation treatment algorithm. Remember the goal in cardiac resuscitation: preventing ischemic brain injury while restoring the normal circulatory action of the heart. When evaluating a possible cardiac patient have your resuscitation medications and equipment set up and ready to go. If the patient goes into arrest, the appropriate action can be taken with a minimum of confusion. Patients with acute myocardial infarctions can go into a malignant arrhythmia (frequently V-Tach or V-Fib) with no warning. Resuscitation Algorithms Cardiac resuscitation algorithms have been developed by the American Heart Association, but could not be reprinted here for copyright reasons. Symptoms result due to low numbers of cells or deficient cell function (which paradoxically may occur with increased numbers of abnormal cells, such as with leukemia), or when cell numbers build up to such a point that they obstruct blood flow. Low cell numbers are caused by decreased production, or increased loss (bleeding), consumption or destruction. Plasma contains the soluble coagulation factors, immunoglobulins, electrolytes, protein and water. Evaluation of blood disorders often requires performing a spun hematocrit and a Wright (Cameco Quick Stain) stained peripheral smear (see Lab Procedures Section). Anemia Introduction: Anemia refers to an abnormally low amount of the oxygen-carrying protein hemoglobin (may also have low number or volume of red cells) in peripheral blood. It is a rough measure of the amount of oxygen-carrying protein (hemoglobin) in the sample, but is subject to many problems with technique that can lead to numbers that do not reflect the true hemoglobin content of blood. Modern Coulter Counters used in clinical labs actually measure the amount of hemoglobin, and calculate, but do not actually measure, the hematocrit. Anemia may be acute (traumatic blood loss) or chronic (due to chronic disease), and results from either increased loss/destruction of red cells or failure of the bone marrow to produce sufficient quantities of hemoglobin/red cells to make up for normal red cell loss. The procedure for obtaining a hematocrit and normal values are specific to the machine used. Normal hemoglobin levels differ among ethnic populations and between men and women, with males and whites averaging higher values. Worldwide, the most common cause of acquired anemia is iron deficiency due to chronic blood loss from hookworm and menstruation. Other important causes are lack of important nutrients (protein, Vitamin B12, Folic Acid) and suppression of the bone marrow from chronic infection or inflammation. The causes of anemia are extensive and beyond the ability of the medic to accurately diagnose in the field environment. Subjective: Symptoms Acute: Lightheadedness, pallor, shock, syncope, altered mental status. Chronic: Lethargy, fatigue and decreased energy, rapid heartbeat and shortness of breath/dyspnea with exertion. Objective: Signs Using Basic Tools: Acute: shock, hypotension, weak pulse, syncope, altered mental status. Increased eosinophils suggest either infection (parasites, especially visceral larval migrans, or chlamydia), hypersensitivity or allergic reactions. Increased basophils are so unusual as to suggest a problem with the stain or staining procedure. Unusual hemoglobins or hemoglobin levels may be common within certain ethnic groups. Iron supplementation is appropriate only for menstruating females and patients whose stool is positive for occult blood, pending further evaluation. Iron supplementation is not otherwise appropriate without laboratory determination of iron deficiency. Blood replacement in the face of rapid loss is addressed in Procedure: Field Transfusion*. Liberal use of medications for pain (Selection of medications is determined by the severity of the pain. Non-steroidal anti-inflammatory drugs like ibuprofen, acetaminophen with codeine, or intravenous morphine are appropriate for mild, moderate and severe pain, respectively, and should be continued until pain levels decrease. Follow-up Actions Evacuation/Consultation Criteria: Evacuate patients with acute anemia and acute sickle crisis after initial stabilization. This section focuses on the relatively mild, viral, acute respiratory tract infections (contrast with Acute Respiratory Distress Syndrome Section later in this chapter), typically called colds. Acute local infections generally occur at the site of viral infection the nose and throat. The flu is a viral infection of the nose, throat, bronchial tubes and lungs caused by inuenza viruses A or B, typically presenting with sudden fever, chills, headache and fatigue. Patients generally continue functioning with a cold virus, but with u their activity is more seriously curtailed. Elderly patients, infants, expectant mothers (3rd trimester) the immunosuppressed and patients with chronic heart and lung diseases will have more frequent life-threatening complications, such as pneumonia. Subjective: Symptoms General: Malaise, fever, nasal congestion, clear secretions, sneezing, scratchy or sore throat, cough, hoarseness, and headache Focused History: Quality: Is your cough productive Allergic rhinitis seasonal history of itching in nose, roof of mouth, throat, and eyes; increased tearing, sneezing and watery discharge; sore throat due to postnasal drip (granular appearance to posterior pharynx); nasal membranes swollen and red. Irritant rhinitis non-seasonal history of exposure to irritant, rhinorrhea without ocular symptoms or sore throat. Mononucleosis positive Monospot; longer illness; higher fever, chills, malaise, sore throat, and swollen cervical lymph nodes. Sinusitis tender sinuses; red, swollen nasal membranes; green or yellow discharge from nose and throat; can follow a cold. Mumps seen typically in children but can attack non-immune adults; swollen salivary glands. Pertussis characteristic whooping cough; seen typically in children but can attack non-immune adults. Diphtheria seen typically in children but can attack non-immune adults; gray membrane maybe seen on pharynx. Adenovirus fever, pharyngitis, and/or conjunctivitis; usually in epidemics in non-immune recruits or displaced persons Strep Pharyngitis palatal petechiae, red beefy uvula, and scarlatiniform rashes are typical for Group A streptococcal pharyngitis. Gonococcal Pharyngitis often asymptomatic, but may have sore red throat, painful swallowing and history of exposure Plan: Treatment 1. See appropriate sections for treatment of pneumonia, infectious mononucleosis, sinusitis and other illnesses that present similarly to cold/flu. Treat cold symptomatically: Rest; fluids (higher insensible losses due to fever); acetaminophen; warm, salt water gargles (sore throat); warm steam from a tea kettle or shower, and saline nasal drops (nasal congestion); no tobacco and alcohol products; hot chicken soup. Antibiotics: Only indicated in patients that may have or are at high risk for a secondary bacterial infection (see pneumonia). Allergic rhinitis: Diphenhydramine Adults and children over 12: 25-50 mg po tid/qid; children under 12: 5 mg/kg/day po in divided doses qid. Irritant rhinitis: Use saline nose drops to lavage nasal mucosa, followed by pseudoephedrine 30-60mg po q4-6h to decrease mucus membrane swelling. Codeine q hs can be used for severe cough and will cause drowsiness (use no more than 3 nights).
Diseases
- Renal carcinoma, familial
- Quinism
- Kaplowitz Bodurtha syndrome
- Angiosarcoma
- Familial hypertension
- Epidermolysis bullosa intraepidermic
- Specific phobia
- Exomphalos-macroglossia-gigantism syndrome
- Triphalangeal thumbs brachyectrodactyly
Buy purim online from canada
Because these specific facts have not been plausibly alleged medications similar to lyrica buy purim 60caps without prescription, the Court shall not permit the estoppel claim to proceed at this time. Plaintiffs ask the Court to enjoin the enforcement of the Accession and Retention Directives pending the final resolution of this lawsuit. The Court finds (1) that Plaintiffs have a likelihood of succeeding on their claim that the Accession and Retention Directives violate the Fifth Amendment, (2) that Plaintiffs would suffer irreparable injury in the absence of an injunction, and (3) that the balance of equities and the public interest favor granting injunctive relief. Level of Scrutiny the general rule is that government action that treats certain classes of people differently is presumed to be valid and will be sustained if the classification drawn. However, this general rule does not apply where the government action draws distinctions between individuals based on certain suspect or quasi-suspect classifications. At this preliminary stage of the case, the Court is persuaded that it must apply a heightened degree of scrutiny to the Accession and Retention Directives. Also relevant is whether the group has been relegated to such a position of political powerlessness as to command extraordinary protection from the majoritarian political process. Finally, the Supreme Court has also considered whether the group exhibit[s] obvious, immutable, or distinguishing characteristics that define them as a discrete group. Transgender individuals have immutable and distinguishing characteristics that make them a discernable class. As a class, transgender individuals have suffered, and continue to suffer, severe persecution and discrimination. See State Amici Brief at 2; Medical Amici Brief at 2; Trevor Project Amici Brief at 9. The exemplary military service of Plaintiffs in this case certainly suggests that it does not. Finally, transgender people as a group represent a very small subset of society lacking the sort of political power other groups might harness to protect themselves from discrimination. See Medical Amici Brief at 4 (noting that recent estimates suggest that transgender individuals make up approximately 0. Ohio 2016) (finding that transgender status is a quasi-suspect class under the Equal Protection Clause); Adkins, 143 F. It is well-established that gender-based discrimination includes discrimination based on non conformity with gender stereotypes. The defining characteristic of a transgender individual is that their inward identity, behavior, and possibly their physical characteristics, do not conform to stereotypes of how an individual of their assigned sex should feel, act and look. By excluding an entire category of people from military service on this characteristic alone, the Accession and Retention Directives punish individuals for failing to adhere to gender stereotypes. A service member who was born a male is punished by the Accession and Retention Directives if he identifies as a woman, whereas that same service member would be free to join and remain in the military if he was born a female, or if he agreed to act in the way society expects males to act. The Accession and Retention Directives are accordingly inextricably intertwined with gender classifications. Before moving on to that analysis, however, the Court pauses to note that meaningful scrutiny of the constitutionality of the Accession and Retention Directives is appropriate despite the fact that they pertain to decisions about military personnel. Circuit has explained that although the operation of the military is vested in Congress and the Executive, and. Under intermediate scrutiny, the government must demonstrate an exceedingly persuasive justification for its actions. At the outset, the Court reiterates precisely what is at issue in this case: a policy banning the accession, and allowing the discharge, of an entire category of individuals from the military solely because they are transgender, despite their ability to meet all of the physical, psychological, and other standards for military service. First, Defendants argue that at least some transgender individuals suffer from medical conditions that could impede the performance of their duties. Second, Defendants argue that there is room for the military to think that certain medical conditions may limit the deployability of transgender individuals as well as impose additional costs on the armed forces. Third, Defendants argue that the President could reasonably conclude that the presence of transgender individuals in the military 9 would harm unit cohesion. Plaintiffs do not dispute that maximizing military effectiveness, lethality and unit cohesion, and even budgetary considerations, are all important or at least legitimate government interests. Based on the combined effect of a number of unusual factors, the Court finds it likely that Plaintiffs will succeed on this claim. First, the reasons given for the decision to exclude transgender service members appear to be hypothetical and extremely overbroad. For instance, Defendants cite concerns that some transgender individuals could suffer from medical conditions that impede their duties, and 9 Plaintiffs note that similar arguments were proffered in support of prior policies precluding service members from being openly gay, maintaining racially segregated ranks and excluding women from military colleges. As an initial matter, these hypothetical concerns could be raised about any service members. Moreover, these concerns do not explain the need to discharge and deny accession to all transgender people who meet the relevant physical, mental and medical standards for service. The Accession and Retention Directives are accordingly extremely overbroad when considered in the light of their proffered justifications. The breadth of the Accession and Retention Directives is also discontinuous with the purported concern about costs, which, in addition to having been found to be minimal or negligible, apparently are primarily related to a surgical procedure that only a subset of transgender individuals will even need. Similarly, Defendants provide practically no explanation at all, let alone support, for their suggestion that the presence of transgender individuals may be harmful to 10 unit cohesion. As far as the Court is aware at this preliminary stage, all of the reasons proffered by the President for excluding transgender individuals from the military in this case were not merely unsupported, but were actually contradicted by the studies, conclusions and judgment of the military itself. As described above, the effect of transgender individuals serving in the military had been studied by the military immediately prior to the issuance of the Presidential Memorandum. The Department of Defense Working Group, made up of senior uniformed officers and senior civilian officers from each military department, unanimously concluded that there were no barriers that should prevent transgender individuals from serving in the military, rejecting the very concerns supposedly underlying the Accession and Retention Directives. In fact, the Working Group concluded that prohibiting transgender service members would undermine military effectiveness and readiness. Next, the Army, Air Force and Navy each concluded that transgender individuals should be allowed to serve. Finally, the Secretary of Defense concluded that the needs of the military were best served by allowing transgender individuals to openly serve. As explained above, after a lengthy review process by senior military personnel, the military had recently determined that permitting transgender individuals to serve would not have adverse effects on the military and had announced that such individuals were free to serve openly.
Generic purim 60caps without prescription
Possible global strategies for stopping polio immunization and how they could be harmonized treatment of hemorrhoids buy purim 60 caps free shipping. An outbreak of poliomyelitis in Israel in 1 961 and the use of attenuated type 1 vaccine in its control. R ecommendations to assure the quality,safety,and efficacy of poliomyelitis vaccines (oral,live,attenuated). W H O collaborative studies on poliovirus type 3 strains isolated during the 1 968 poliomyelitis epidemic in Poland. The role of virologic surveillance in the global initiative to eradicate poliomyelitis. Q uasispecies diversity determines pathogenesis through cooperative interactions in a viral population. M assively parallel sequencing for monitoring genetic consistency and quality control of live viral vaccines. Consistent selection of mutations in t h e 5 untranslated region of oral poliovirus vaccine upon passaging in vitro. R ational design of genetically stable,live attenuated poliovirus vaccines of all three serotypes:relevance to poliomyelitis eradication. M odulation of poliovirus replicative fitness in H eLa cells by deoptimization of synonymous codon usage in the capsid region. R eduction of the rate of poliovirus protein synthesis through large-scale codon deoptimization causes attenuation of viral virulence by lowering specific infectivity. A recombinant virus between the Sabin 1 and Sabin 3 vaccine strains of poliovirus as a possible candidate for a new type 3 poliovirus live vaccine strain. Construction of less neurovirulent polioviruses by introducing deletions into the 5noncoding region of the genome. M odification of translational control elements as a new approach to design of attenuated picornavirus strains. Genetic inactivation of poliovirus infectivity by increasing the frequencies of CpG and U pA dinucleotides within and across synonymous capsid region codons. Increased fidelity reduces poliovirus fitness and virulence under selective pressure in mice. T ransitory appearance of type 2 neutralizing antibody in patients infected with type 1 poliomyelitis virus. Possible protective effect of previous type 2 infection against paralytic poliomyelitis due to type 1 virus. Antibody response to varicella-zoster virus after natural and vaccine-induced infection. Studies on the immunogenicity, communicability and genetic stability of oral poliovaccine administered during the winter. S e r o l ogic response to oral polio vaccine and enhanced-potency inactivated polio vaccines. R esponse to an Infant Immunization Schedule Combining Oral and Inactivated Poliovirus V accines Compared With Either V accine Alone:R esults of a R andomized T rial in The Gambia,Oma n, and T hailand. Combined immunization of infants with oral and inactivated poliovirus vaccines:results of a randomized trial in The Gambia,Oman,and T hailand. W orld H ealth Organization Collaborative Study Group on Oral Poliovirus V accine. Factors affecting the immunogenicity of oral poliovirus vaccine:a prospective evaluation in Brazil and The Gambia. Z inc supplementation fails to increase the immunogenicity of oral poliovirus vaccine:a randomized controlled trial. Effect of buffer on the immune response to trivalent oral poliovirus vaccine in Bangladesh:a community based randomized controlled trial. Immunogenicity of poliovirus vaccines in chronically malnourished infants:a randomized controlled trial in Pakistan. Poliovirus antibody titres,relative affinity,and neutralizing capacity in maternal milk. Immunologic aspects of human colostrum and milk: interaction with the intestinal immunity of the neonate. Protective efficacy of a monovalent oral type 1 poliovirus vaccine:a case-control study. Polio eradication:surveys of routine immunization coverage and seroprevalence against polioviruses,Y ogyakarta Province,Indonesia. Immunogenicity of bivalent types 1 and 3 oral poliovirus vaccine:a randomised,double-blind,controlled trial. Advisory Committee on Poliomyelitis Eradication: recommendations on the use of bivalent oral poliovirus vaccine types 1 and 3. Immunogenicity of three doses of bivalent, trivalent,or type 1 monovalent oral poliovirus vaccines with a 2 week interval between doses in Bangladesh:an open-label,non-inferiority,randomised,controlled trial. Preexisting poliovirus-specific IgA in the circulation correlates with protection against virus excretion in the elderly. Asymptomatic wild-type poliovirus infection in India among children with previous oral poliovirus vaccination. R esults of a study of the reactogenic and immunogenic properties of live antipoliomyelitis vaccine. The trend of acquired immunity with live poliovirus vaccine and the effect of revaccination:follow-up of vaccinees for ten years. Properties of a new type 3 attenuated poliovirus,V I: alimentary tract resistance in children fed previously with type 3 Sabin vaccine to reinfection with homologous and heterologous type 3 attenuated poliovirus. M ucosal immunity induced by enhanced potency inactivated and oral polio vaccines. R eport of the Second M eeting of the G l o ba l Commission for the Certification of the Eradication of Poliomyelitis,Geneva,1 M ay 1 997. W aning intestinal immunity following vaccination with oral poliovirus vaccines in India. Distribution of echovirus antibody in serum,nasopharynx,rectum and spinal fluid after natural infection with echovirus type 6. Cleavage of V P1 and modification of antigenic site 1 of type 2 polioviruses by intestinal trypsin. Some results of the work on mass immunization in the Soviet U nion with live poliovirus vaccine prepared from Sabin strains. Certification of poliomyelitis eradication: W estern Pacific R egion,October 2000. Large-scale use of S abin type 2 attenuated poliovirus vaccine in Singapore during a type 1 poliomyelitis epidemic. The influence of natural and artificially induced immunity on alimentary infections with polioviruses. Clinical investigations of attenuated strains of poliomyelitis virus:use as a method of immunization of children with living virus. Oral poliovirus vaccine (Sabin)in Czechoslovakia:effectiveness of nationwide use in 1 960. In: Proceedings of the First International Conference on Live Poliovirus V accines. Enterovirus surveillance following a community-wide oral poliovirus vaccination program:a seven-year study. Live,orally given poliovirus vaccine:effect of rapid mass immunization on population under conditions of massive enteric infections with other viruses. Seroprevalence of antibody against poliovirus in inner-city preschool children:implications for vaccination policy in the U nited States. Antibody response and viral excretion after live polio vaccine or a combined schedule of live and inactivated polio vaccines.
Cheap purim 60 caps amex
There is a continuous (machinery) murmur with systolic accentuation medicine technology buy cheap purim 60 caps online, maximal in the second left intercostal space and Assessment posteriorly. Ostium primum: usually, there is left axis deviation Assessment with evidence of right ventricular hypertrophy. Echocardiography shows a dilated left atrium and monary circulation left ventricle. The typical murmur is of pulmonary stenosis with a may be dyspnoea and bronchitis. Chest X-ray shows a normal-sized but boot-shaped (and thrill) is present in the fourth left intercostal heartandalargeaortawithasmallpulmonaryartery space. The patient becomes cyanosed and deteri orates rapidly with symptoms of dyspnoea, syncope Management and angina. Coarctation of the aorta Infective endocarditis these represent 5% of congenital heart disease cases. Ninety-eight percent are distal to Heart valves are infected as part of an acute septicae the origin of the left subclavian artery. It follows in fection with staphylococcus, often in association with Signs indwelling intravenous catheters or primary infection of the lungs or skin. The murmurs are: T a systolic murmur at front and back of the left Predisposing abnormalities upper thorax T collateral murmurs over the scapulae. Acquired: rheumatic valve disease now accounts for obscured by the coarctation murmur. Mitral valve prolapse, calcied aortic stenosis and syphilitic aor Assessment titis (rare) predispose to endocarditis. There is rib notching (and notching at the scapular margin) and Organisms normal or large cardiac shadow. The origin of infection varies with the infecting or Associations ganism and includes teeth and tonsils (Streptococcus viridans), urinary tract and bowel (S. Management Percutaneous intervention (angioplasty with or with Diagnosis out stenting or surgical correction). The diagnosis of infective endocarditis should be considered in any patient with a predisposing cardiac lesion who develops any illness. The most efficient Eisenmenger syndrome way to establish the diagnosis is by: There is a reversal of a left-to-right shunt. It also frequently causes endo the symptoms and signs may be considered in three carditis in patients with insulin-dependent diabetes groups. A wide spectrum of organisms can infect 1 Signs of general infection: lethargy, malaise, anae prosthetic valves. Gram-positive and Gram-negative mia and low-grade fever are frequent but not in bacilli are relatively uncommon causative organisms. There may be curs in patients with prosthetic valves, compromised transientmyalgiaor arthralgia. Therapy should be continued for at least 4 weeks 2 Signs of underlying cardiac lesions must be sought. The patient suggestive and the patient must be examined for should be carefully followed for recurrence. The diagnosis depends on nding a rise in antibody Immune complexes are present in serum and com titre. Episodesofinfectioninpeopleatrisk of infective endocarditis should be investigated and Aetiology treated promptly. It may be caused by tuberculosis followingspreadfromthepleuraormediastinallymph Chemotherapy glands. It may follow acute viral or pyogenic pericar It is essential to obtain blood culture before starting ditis, but the cause is often unclear. Antibiotic therapy is guided by identi dium, irradiation and carcinoma account for a few cationofthecausativeorganism,butitshouldnotbe cases. It may be simulated by restrictive cardiomyop delayed in the presenceof good clinical evidence even athy (p. Acute benign pericarditis often fol Symptoms result from cardiac constriction with de lows a respiratory infection and is probably viral. Right heart rising antibody titre to Coxsackie B virus is sometimes failurepredominatesoverleft. It results from little or no ankle swelling are characteristic, but dys infection with staphylococcus or, occasionally, hae pnoea and ankle swelling may occur later. The liver, and sometimes There may be pain referred to the left shoulder if the the spleen, is enlarged. A the signs of pericardial effusion without tampo third sound, brought about by an abrupt end to ven nade are an absent apex beat, a silent heart and tricular lling, may be present. TheparadoxthatKussmaulnotedwasthatthe ChestX-ray:theremaybecalcicationofthepericar heart continued to beat strongly while the peripheral dium (often seen only in the lateral lm). Effusion classically produces an enlarged pear shapedcardiacshadowwith lossof normalcontours. Echocardiography is the most sensitive way of de tecting pericardial uid with free space between the Acute pericarditis heart and pericardium. Aetiology Management Pericarditis is common within the rst week of Aspirate for tamponade (if the systolic arterial blood acute myocardial infarction. It is treated by insertion of a drain or creation of a peri characterised by fever, pleurisy, and pericarditis. Cardiovascular disease 107 Management Syphilitic aortitis and b-blockade is given to increase left ventricular com plianceandreducetheincidenceofdysrhythmias and carditis angina. Pa the aorta, the aortic ring to produce dilatation or tients who develop atrial brillation should be antic aneurysm, and aortic regurgitation and the coronary oagulated and digoxin can be added. Patients should receive genetic counselling and screening of their families should be offered. It is usually restricted to cardiomyopathies of unknown Dilated (congestive) cause or association. They are classied into three major groups depending upon the clinical effects of cardiomyopathy the abnormality on the left ventricle, which may be: this is very rarely familial. Byconvention,themorecom mon and more easily diagnosed myocardial disorders Hypertrophic are excluded, i. Angina,systemicandpulmonary cardiomyopathy infarcts, conduction defects and arrhythmias occur. There is a steep-rising, jerky pulse (unlike the slow rising, plateau pulse of aortic valve stenosis), car Management diac hypertrophy, a palpable atrial beat followed by a late systolic aortic ejection murmur, usually Heart failure should be treated (p. Anticoagulants heard best in the left third and fourth intercostal are given because of the risks of embolism. Diagnosis Pain (usually severe) is associated with numbness, Intermittent claudication paraesthesiae and paresis. The limb becomes anaesthetic and the ar mellitus and hyperlipidaemia, and occasionally terial pulses weak or absent. Obstruction is most com monly femoropopliteal, and less often aortoiliac or Management distal. Treatment should involve vascular surgeons and radiologists, and approaches include anticoagula Diagnosis tion and antiplatelet agents, thrombolytic agents the history is of pain in the calf on effort with rapid and embolectomy, angioplasty and arterial bypass relief by rest. There may Ischaemic foot be cyanosis, pallor or redness, oedema, ulcers or this is usually caused by chronic arterial obstruction gangrene. Arteriography is diabetes and is associated with neuropathy and local required if surgery is contemplated. The feet are cold and Exercise within the effort tolerance to help develop pulses diminished or are absent.
Padmoj (Lotus). Purim.
- How does Lotus work?
- Bleeding, digestion problems, diarrhea, and other conditions.
- Are there safety concerns?
- What is Lotus?
- Dosing considerations for Lotus.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96164
Buy genuine purim online
As an alternative to the wire scalpel treatment for plantar fasciitis 60caps purim otc, we used a 20-gauge metal type spinal needle cannula (Hakko Co. This technique is less expensive than the use of a wire scalpel and easily available when needed. Therefore, on the basis of favorable results, our modified subcision technique may be considered effective for prominent nasolabial fold correction. Abstract the arthroscopic treatment of the "bony Bankart lesion" continues to evolve. We present a novel technique that we developed at Orthopaedic Research of Virginia, the "transosseous bony Bankart repair," which incorporates several essential concepts to provide for optimal healing and rehabilitation. We promote arthroscopic repair emphasizing bone preservation, a fracture interface without interposing sutures, the ability to reduce capsular volume, and multiple points of stable glenolabral fixation. Our technique positions suture anchors within the subchondral bone of the intact glenoid to allow for an anatomic reduction of the bony fragment. By use of an arthroscopic drill, spinal needle, and nitinol suture passing wire, the sutures are passed in a retrograde fashion through the bony Bankart fragment and anterior capsule in a mattress configuration. Additional inferior and superior anchors are placed to further provide stability and reduce capsular volume. While maximizing fracture surface area and optimizing bony healing, the end result is an anatomic reduction of the bony fragment and the glenoid articular surface. Abstract Infra-patellar fat pad cysts are an uncommon type of intra-articular ganglia. We report a case of a young woman with a painful little mass in the anterior aspect of the left knee. Ultrasound revealed a multiloculate cyst, that was initially drained with a spinal needle. Four months later, she had a recurrence of symptoms and a ultrasound guided aspiration was performed. Cytological examination revealed synovial cells, synovial fluid, macrophages and debris: diagnosis was ganglion cyst. Clinical diagnosis of an intraarticular cyst is very difficult, but sometimes an infra-patellar fat pad cyst could be suspected because it could be visible and palpable. In our opinion ultrasound guided aspiration is the treatment of choice in symptomatic ganglia, because it allows to drain all lacunae, preventing recurrence. Topographic description of an alternative insertion technique for percutaneous approach of cricopharyngeus muscle electromyography: a cadaveric and clinical study. Source Department of Anatomy, Cerrahapasa Medical Faculty, Istanbul University, Istanbul, Turkey. Because of some practical difficulties, electrophysiologic tests for this muscle are not performed routinely. Thus we aimed to describe an alternative topographic way to reach the muscle easily. The needle was inserted percutaneous at the level of the superior border of the cricoid cartilage, anterior to the anterior border of the sternocleidomastoid muscle at 60 degrees angle to the frontal plane in the posteromedial direction. In all of the patients, the needle entered the muscle on the first attempt; that was confirmed by electromyographic responses. Macrolane (large particle biphasic hyaluronic acid) filler injection for correction of defect contour after liposuction. Abstract Abstract In a minority of patients undergoing liposuction, superficial irregularities (or skin depression) in the operated area may occur. In this study, the authors investigated the effectiveness, maintenance, and safety of Macrolane as a "non-surgical" treatment to correct skin depression after liposuction. Macrolane was injected at a subdermal superficial plane using an intramuscular or spinal needle. At 8 months post-injection, a persistence of correction of 60-70% was still present in 90% of the patients. In conclusion, Macrolane filler injections are a predictable, safe, and long-lasting non-surgical procedure to fill contour defects that arise after liposuction, and represent a good option for patients who refuse to undergo an additional surgery to fill the arisen skin depressions. Indications of 1342 fetal cord blood sampling procedures performed as an integral part of high risk pregnancy care. Source Department of Obstetrics & Gynecology, All India Institute of Medical Sciences, Room No 3073, 3rd Floor Teaching Block, Ansari Nagar, New Delhi, 110029 India. Awareness of feasibility of the procedure and indications for the same should be known to every obstetrician. Under continuous ultrasound guidance, a 22 gauge long spinal needle was inserted through the maternal abdomen and uterine wall into the umbilical cord, and about 2-4 ml of blood, depending on the indication was aspirated by syringe. Awareness of the procedure and indications for the same should be known to every obstetrician as it is technically feasible, expertise is available in India; so that women who require the procedure may be referred in time. Laparoendoscopic transgastric histoacryl injection of gastric varices: a new surgical approach. Source Gastrointestinal Surgical Unit, General Surgery Department, Faculty of Medicine, University of Alexandria, Alexandria, Egypt. Endoscopic histoacryl injection is the standard treatment in Egypt; however, because of technical difficulties it is possible to inject only a little amount of this material, as it may endanger the channels of the flexible endoscope. After the patient was placed under general anesthesia, a small gastrostomy was done in the anterior gastric wall through which a 10-mm trocar was inserted for the laparoscopic camera. Use of this procedure is recommended in patients fit for surgery and those who had failed endoscopic injection sclerotherapy. Digital subtraction angiography does not reliably prevent paraplegia associated with lumbar transforaminal epidural steroid injection. An 80-year-old man with severe lumbar spinal stenosis and chronic L5 radiculopathic pain was evaluated at a university pain management center seeking symptomatic pain relief. Foraminal placement of the needle tip was confirmed with anteroposterior, oblique, and lateral views on fluoroscopy. Digital subtraction angiography was performed twice to confirm the absence of intravascular contrast medium spread. Two minutes later, a mixture of one mL of 1% lidocaine with 80 mg triamcinolone acetonide was injected. Immediately following the completion of the injection, the patient reported extreme bilateral lower extremity pain. He became diaphoretic, followed by marked weakness in his bilateral lower extremities and numbness up to his lower abdomen. It showed a small high T2 signal focus in the thoracic spinal cord at the T7-T8 level. The patient was admitted to the critical care unit for neurological observation and treatment with intravenous methylprednisolone. At discharge to an acute inpatient rehabilitation program, the patient had persistent bilateral lower extremity paralysis, and incontinence of bowel and bladder functions. Utilizing blunt needles or larger bevel needles in place of sharp, cutting needles may minimize the chances of this event occurring. Surgical technique: arthroscopic treatment of heterotopic ossification of the hip after prior hip arthroscopy. There were 36 females and 30 males with an average age of 38 years (range, 15-68 years). The minimum followup for the three patients with revision surgery was 2 years (mean, 2 years 2 months; range, 2 years-2 years 8 months). In symptomatic patients, arthroscopic excision appears to relieve pain and restore function Orthop Surg. Source Department of Orthopaedic Surgery, Istituto Chirurgico Ortopedico Traumatologico, Latina, Italy. These techniques seem to be difficult challenges for the majority of arthroscopic surgeons, and because of that they are called "highly demanding" techniques. Without the use of dedicated instruments and cannulas, the authors propose a V-sled technique that seems to be more reproducible, quicker and less difficult to perform for arthroscopic shoulder surgeons. In addition, two free high strength sutures are passed through the muscle, respectively. The third wire from each anchor is retrieved out of the accessories portals used for the insertion of the anchors. In addition, two free high strength sutures are passed through the muscle, and the patch sizing is done using a measuring probe introduced through the lateral portal. Next, the patch is then prepared and is introduced into the subacromial space, and then the patch is stabilized, and the free sutures are tied. Patients with previous labral resection or Tonnis grade greater than 1 were excluded.
Buy line purim
Most of it is cleared by the liver symptoms flu generic purim 60 caps amex, but a minor part reaches the systemic circulation and can be excreted by the kidneys. Measurement of urobilinogen in urine has been used to differentiate between different forms of icterus and cholestasis. However, due to many physiologic variations and technical errors, this parameter has no clinical value. Bilirubin is cleared from the blood, conjugated, and excreted into bile by the liver. The clearance is not an efficient process18,19 in contrast to the hepatic clearance of bile acids. Whereas bile acids are nearly completely cleared during the first passage, bilirubin requires many passages to become cleared completely. As a conse quence, bilirubin is equally distributed over the entire circulation, but bile acids are highly concentrated in the portal blood and have a low concentration in the systemic circulation. This explains the differences in the reaction pattern of bilirubin and bile Clinical Syndromes Associated with Liver Disease 423 Ineffective clearance and recirculation Complete clearance bilirubin in 1 circulation Bile acids gut. Bile acids are reabsorbed and undergo an enterohepatic circulation, which is maintained by an efficient clearance of bile acids from the portal vein. Bilirubin is not absorbed from the small intestines and its hepatic clearance from the blood has low efficiency. Consequently, there is a high gradient between the portal and systemic concentrations of bile acids, but not of bilirubin. Furthermore, systemic bile acids are increased due to portosystemic shunting and cholestasis; bilirubin is only increased due to cholestasis (or increased production in case of severe hemolysis). In diseases with cholestasis, all bile components including bilirubin and bile acids gain entry to the systemic circulation with the hepatic lymph. This process is not related to hepatic clearance or portal perfusion of the liver. Conversely, in diseases characterized by portosystemic shunting (congenital porto systemic shunts, portal hypertension, acquired collateral circulation, and so forth), the high portal bile acid concentration reaches the systemic circulation giving a high plasma bile acid concentration. However, the bilirubin concentration is not influenced by abnormal liver perfusion. The main processes by which plasma bilirubin may increase are increased produc tion and cholestasis. An increased level becomes clinically visible only as icterus (yellow discoloration of sclerae, mucous membranes and skin) when the concentration exceeds 15 mmol/L. Due to the huge liver reserve capacity, most patients remain in the subclinical region and do not become icteric, despite the fact that nearly all nonvascular liver diseases leadto somedegreeofcholestasis. Given the 2 main reasons for hyperbilirubinemia, increased production and chole stasis, measurement of unconjugated and conjugated bilirubin has been used as an expression of these 2 processes. However, with sensitive techniques, it has been shown that hemolytic (increased production) and hepatobiliary diseases (cholestasis) are not different with respect to the fraction of unconjugated bilirubin, which always 424 Rothuizen varies between 15% and 40%. In liver diseases, there is considerable hemolysis (eg, due to portal hypertension causing reduced splanchnic blood flow with prolonged trapping and degradation of red blood cells in the spleen, and altered erythrocyte membrane fluidity caused by high plasma bile acid concentrations). Furthermore, animals with liver disease may have increased bilirubin production from hepatocyte hemoproteins. Hepatic and hemolytic diseases also have comparable reductions of the bile flow as an expression of cholestasis. With mild anemia, the liver is not damaged and the reserve capacity of the liver prevents such patients from becoming icteric. As hepatic and hemolytic jaundice always consist of a mixed type of hyperbilirubinemia, the measurement of unconjugated and conjugated bilirubin is clinically useless. Furthermore, if only severe hemolysis leads to jaundice, such animals should have pale mucous membranes (and hematocrit <20%). Moderately pale or normally colored mucous membranes in the presence of icterus immediately indicate the presence of a primary disease of the liver or biliary tract. Conjugated bilirubin in plasma binds covalently (irreversibly) to protein albumin. This bilirubin can only escape the circulation when albumin becomes catabolized; its half-life is about 2 weeks. Therefore, after complete recovery from the underlying cholestatic disease, icterus may remain for several weeks and does not necessarily reflect the actual situ ation, which may be important when evaluating the effect of therapy. Portal hypertension can be caused by an increased delivery of blood to the portal system, or by an increased resistance to the passage of portal blood. An increased delivery of blood occurs animals with arteriovenous shunts in the splanchnic circulation, usually in the liver, causing the direct connection of the arterial blood pressure with the portal system. Usually, however, portal hypertension is caused by an increased resistance to the portal blood stream. The cause can be prehepatic (in the portal vein itself), intrahepatic, or posthepatic (hepatic veins, caudal vena cava, heart). Posthepatic causes have little influence on the liver functions, but increased hydrostatic portal blood pressure may cause ascites. Most cases of clinically relevant portal hypertension have a cause inside the liver. Liver diseases causing portal hypertension give rise to different liver Clinical Syndromes Associated with Liver Disease 425 dysfunctions, such as reduced protein and albumin production. However, even in severe liver dysfunction, the capacity of the liver to produce proteins is only moder ately affected due to the large plasticity of the liver. Therefore, albumin levels usually do not fall below 18 to 20 g/L, which is more than the concentration that, by itself, may cause edema and ascites (<15 g/L). However, the combination of portal hypertension and moderate hypoalbuminemia often produces ascites in such animals. The hindrance to the portal circulation develops by way of compression of the portal veins in the portal and periportal area of the liver lobules. Because the cause lies at the site of entry of blood into the liver lobules, the liver itself is not congested. Due to loss of functional tissue, most of these diseases are associated with an abnormally small liver. The most frequent cause of portal vein compression is deposition of collagen (fibrosis)23,24 and infiltration of inflammatory cells (chronic hepatitis). In advanced cases, cirrhosis, defined as disruption of the normal lobular architecture of the liver by fibrous tissue, occurs. Then, resistance to the portal blood flow occurs at different levels of the lobule and is most severe. Portal vein hypoplasia (formerly called microvascular dysplasia) is associated with variable degrees of liver fibrosis, which may increase the resistance to normal liver perfusion. Posthepatic causes of portal hypertension may be localized in the inferior vena cava and the heart. Obstruction of the hepatic veins either intra or extrahepatic (Budd Chiari syndrome and veno-occlusive disease, respectively) occur in other species, but not in cats or dogs. Thrombosis of the inferior vena cava is rare, and is often caused by an adrenal tumor giving local thrombophlebitis. Such a thrombus grows out in the direc tion of the blood stream and may occlude the lumen over a long distance. In posthe patic causes of portal hypertension the liver is congested and enlarged. Liver functions, however, remain adequate and biochemical examination usually reveals no or only slight liver cell damage and dysfunction. If disorders affecting the afferent portal system cause reduced perfusion of the liver, there is secondary hypoplasia of the portal veins and increased growth of tortuous hepatic arteries (arterialization) in the portal areas. With the exception of congenital shunts, all of these diseases cause increased resistance for the portal blood flow through the liver, and therefore portal hypertension.
60 caps purim for sale
It is spread by fecal-oral transmission or ingesting vegetables contaminated with whipworm eggs 4 medications walgreens buy purim 60caps otc. Infection is generally asymptomatic, but patients with heavy worm burdens may present with anemia, bloody diarrhea, growth retardation or rectal prolapse. Subjective: Symptoms Usually asymptomatic; may have abdominal pain, bloody diarrhea, malaise, and rectal prolapse. Differential Diagnosis: Bloody diarrhea/anemia amebiasis, shigellosis and inammatory bowel disease. Plan: Treatment: Primary: Albendazole 400 mg po for one dose Alternative: Mebendazole (Vermox) 100mg bid x 3 days Patient Education Prevention: Avoid uncooked vegetables in endemic areas. Subjective: Symptoms A painful trypanosomal chancre may develop at the site of the tsetse fly bite. West African: Fever develops weeks to months after the bite, followed by lymphadenopathy. The final phase is marked by progressive neurologic impairment ending in coma and death. East African: the onset of symptoms usually occurs more rapidly, with fever, malaise and headache occurring within a few days to weeks. Using Advanced Tools: Trypanosomes may be seen on examination of thick and thin peripheral blood smears. Differential Diagnosis: Fever many other diseases can cause similar symptoms, including tuberculosis and malaria. A history of travel to an area endemic for African Trypanosomiasis should prompt a diagnostic evaluation for that disease. Altered mental status meningitis, brain abscess Plan: Treatment: Requires evacuation to a medical center with infectious disease and tropical medicine support for definitive diagnosis and treatment. Medications: Since medications have several severe side effects, they should only be given at a tertiary care center. Follow-up Actions Consultation Criteria: All suspected cases should be referred for consultation. Zoonotic Disease Considerations Principal Animal Hosts: Dogs, ruminants, carnivores Clinical Disease in Animals: Intermittent fever, anemia, weight loss; may be asymptomatic. Chronic: Years later: heart failure; enlargement of the esophagus or colon Focused History: Do you recall an unusual, red, swollen insect bite or swelling around one eye Using Advanced Tools: Lab: Parasites in peripheral blood smears (thick and thin) can be found during febrile periods early in the course of infection. Prevention and Hygiene: Avoid insect bites and infested areas; wear protective clothing. Zoonotic Disease Considerations Principal Animal Hosts: Dogs, cats, rodents Clinical Disease in Animals: Intermittent fever, anemia, weight loss; may be asymptomatic Probable Mode of Transmission: Contaminated bite wounds or contact with fecal matter of Reduviidae family of insects (kissing bugs). Extrapulmonary disease occurs in approximately 15% of infected persons and can affect virtually any organ system (see Skin: Cutaneous Tuberculosis) and can disseminate throughout the body. Subjective: Symptoms Chronic productive cough (bloody), chest pain, fever, chills, night sweats, anorexia, weight loss, fatigue. Plan: Treatment Primary: Base the selection of antimycobacterial drugs on knowledge of local resistance patterns. Patient Education General: Comply with the medication regimen to avoid developing active disease, and then spreading it to others. Evacuation/Consultation Criteria: Evacuation not necessary unless clinically unstable or patient develops significant medication side effect. Consult with pulmonologist, infectious disease specialist or primary care physician prior to treatment and as necessary. Zoonotic Disease Considerations Agent: Mycobacterium bovis Principal Animal Hosts: Cattle Clinical Disease in Animals: Progressive emaciation, lethargy, weakness, anorexia, low-grade fever; chronic bronchopneumonia with moist cough, progressing to tachypnea and dyspnea. Probable Mode of Transmission: Ingestion, inhalation (occupational exposure to farmers) Known Distribution: Worldwide; rare in N. Pulmonary syndromes are usually chronic, often occurring in persons with other underlying pulmonary disease. Subjective: Symptoms Lymphadenitis (painless enlargement of the lymph nodes of the neck), usually unilaterally; skin and soft tissue infections edema, erythema; pulmonary infection chronic, productive cough with fever and weight loss; accompanied by malaise, night sweats and hemoptysis. Other Syndromes: Therapy based on site of disease, organism and susceptibility testing results. No Improvement/Deterioration: Reevaluation and repeat culture and susceptibility testing. Follow-up Actions Wound Care: Local care (clean, dry, protect, topical antibiotics) to prevent secondary bacterial infection. Consultation Criteria: Management of chronic pulmonary infection usually requires specialty consultation. Although the acid-fast bacilli can be detected in lesional or sputum smears or biopsy material, culture is required to confirm diagnosis. Cryptococcosis is found worldwide but symptoms are most common in the immunosuppressed and are not acutely life-threatening. Blastomycosis, coccidioidomycosis, histoplasmosis, and paracoccidioidomycosis are endemic fungal infec tions that should be included in a differential diagnosis so individuals with potential infections may be removed or referred to higher echelons of care. In adults, disease commonly occurs in diabetics, the immunocompromised, and after antibiotic treatment for other disorders. Disseminated, life-threatening infection can also occur in severely immunocompromised persons. Subjective: Symptoms Oral thrush: Usually asymptomatic; may cause mouth discomfort or difficulty swallowing. Vaginal thrush: Itching, dyspareunia (pain with intercourse) and change in the odor or consistency of vaginal discharge. Cutaneous (intertrigo or vulvar): erythematous, shiny rash with small satellite lesions at its periphery. Intertrigo nystatin powder or clotrimazole or miconazole cream twice daily until resolved. Alternative: Oropharyngeal candidiasis clotrimazole troches (lozenges), 10 mg 5/day, oral fluconazole, 50-200 mg/day, itraconazole, 100-200 mg/day, or ketoconazole, 200 mg/day. Esophageal candidiasis itraconazole 100-200 mg/day, or intravenous amphotericin B, 0. Patient Education General: this is a superficial infection that should resolve with standard therapy. It can occur in healthy people, but could indicate other disease such as diabetes or immunocompromise. Medications: Topical antifungals have virtually no adverse effects associated with their use. The oral azoles, fluconazole, itraconazole, and ketoconazole are all well tolerated. These drugs may interact with other drugs processed through the liver, causes the levels of drugs such as oral diabetes, seizure, and anticlotting medications. Ketoconazole that is used long-term may affect steroid hormones, causing irregular menses in women and decreased libido or breast tissue enlargement in men. Malaise, nausea, vomiting, weight loss, and infusion site phlebitis (vein inflammation) may also occur. Intravenous use of amphotericin B is associated with infusion-related fever, headache, chills, myalgias, and rigors. Prevention and Hygiene: None necessary No Improvement/Deterioration: Further evaluation is necessary if infection does not resolve within two weeks. Follow-up Actions Return evaluation: If lesions do not resolve consider alternate treatment. However, those with recurrent thrush, disseminated infection or who require intravenous amphotericin B therapy should be referred to the appropriate higher echelon of care. Most individuals seeking care for this infection have progressive pulmonary disease or cutaneous lesions. Subjective: Symptoms Acute pulmonary infection produces fever, cough, and pleuritic chest pain. Chronic pulmonary disease can also include hemoptysis, weight loss, and skin lesions. These begin as red papules or nodules that enlarge and then ulcerate or become verrucous.
Cheap 60 caps purim amex
There is no known cure for osteogenesis imperfecta; therefore treatment quincke edema purim 60 caps low price, treatment is still supportive and palliative. Achondroplasia is a defect in the formation of cartilage at the epiphyses of long bones, which results in a form of dwarfism sometimes seen in rickets. Persons with achondroplasia will have a normal trunk size (thorax, abdomen, and pelvic cavity) but abnormally shortened extremities. Osteopetrosis is a hereditary condition characterized by excessive calcification of bones resulting in spontaneous fractures and a marble like appearance. Imaging Studies Conventional radiographic examination remains the most useful means of studying the dysplastic skeleton. Inflammatory Conditions & Infections of Bone Inflammatory conditions and infections can either directly or indirectly impact the integrity of the bony skeleton. Inflammation is a process in which the white blood cells release chemicals to protect the body from foreign substances such as bacteria and viruses. When inflammation occurs, chemicals from the white blood cells are released into the blood or 148 affected tissue in an attempt to rid the body of the foreign substance. This chemical release increases blood flow to the area causing redness and warmth. Some chemicals cause leakage of fluid into the tissues, resulting in swelling, which can stimulate nerves, and ultimately causes pain. Many inflammatory conditions affect women and minorities disproportionately, both in increased numbers and increased disease severity. Rheumatoid arthritis, osteoporosis, and osteoarthritis (in patients over 45 years of age) are also more prevalent among women, whereas certain forms of ankylosing spondylitis 2 occur more frequently in men. Rheumatologists have long recognized the incidence of many rheumatic diseases within families and certain ethnic populations, pointing to some role of genetic 2 risk. The perseverance of scientists in gathering biospecimens and clinical histories from patients and their relatives, along with the explosion of knowledge and techniques 2 in genetics, have opened new avenues of research. Genome-wide association studies have transformed the discovery of gene regions, or loci, related to disease risk, through 2 unbiased analyses of patients with a disease compared to controls without it. Association linkage studies have yielded important insights into complex rheumatic 2 disorders, such as lupus, rheumatoid arthritis, and ankylosing spondylitis. Current research also has revealed common genetic factors contributing to other autoimmune 2 diseases as well as co-morbidities. Inflammatory arthritides Inflammatory arthritides are diseases of the synovium and lead to erosive changes of the adjacent bones. Degenerative arthritis/osteoarthritis is secondary to articular cartilage damage from repetitive microtrauma that occurs throughout life. Other factors in degenerative arthritis include heredity, nutrition, metabolic factors, preexisting articular disease, and body habitus. Osteoarthritis most often affects the proximal and 149 distal interphalangeal joints of the hands and the major weight-bearing joints, the hips and the knees, Figure 5-1. The carpal joints at the base of the thumb and the first metatarsophalangeal joint of the foot are commonly affected by degenerative arthritis. Any joint damaged by trauma that results in an irregular articular surface can become prematurely arthritic and produce nodes. Arthroses may be classified into 4 basic groups based on their common characteristics. Rheumatoid arthritis is common in the carpal and tarsal bones and their associated joints. Usually the metacarpophalangeal and the metatarsophalangeal joints are affected first. Septic arthritis is the infection of a joint and is demonstrated on radiography images by a widening of the joint space secondary to joint effusion. Advancements in musculoskeletal imaging allow clinicians to accurately monitor arthritic disease conditions and to determine the effectiveness of drug therapies. An imaging examination offers the clinician insight to make the initial clinical diagnosis. Conventional non-contrast radiography has traditionally been useful in identifying structural damage. Radiography provides the clinician with information about the possible causes of joint pain and swelling, such as that associated with trauma, skeletal abnormalities, infection and tumors. One of the major disadvantages of radiography is that it cannot demonstrate synovial hyperplasia in a joint; thus is limited on the information that can be gleaned about the amount of inflammatory change occurring in the joints. Osteoarthritis Osteoarthritis is the most common type of arthritis and the percentage of people affected increases with age. By 2030, 20% of Americans, or about 72 million people, will th 5 have passed their 65 birthday and will be at risk for the disease. Although osteoarthritis is more common in older people, younger people can develop it; usually as a result of a joint injury, joint malformation, or genetic defect in the joint cartilage. Both men and women have the disease but before age 45, more men 6 than women have osteoarthritis. It is also more likely to occur in people who are overweight and in those whose jobs or leisure activities puts stress on particular joints. Osteoarthritis most often occurs in the hands 6 (at the ends of the fingers and thumb), spine (neck and lower back), knees, and hips. Osteoarthritis, also known as degenerative arthritis and degenerative joint disease, is a condition in which low-grade inflammation results in pain in the joints. The condition destroys or decreases the synovial fluid that lubricates the joints and as the bone surfaces become less well protected by cartilage, the individual experiences pain upon weight bearing, including walking and standing. Healthy cartilage allows bones to glide over one another and it also absorbs energy from the shock of physical movement. Cartilage is a type of connective tissue composed of cells called condrocytes that are embedded in a matrix strengthened with fibers of collagen. Cartilage supports body tissues and provides a cushion type effect for the joint spaces. Over time, the joint may lose its normal shape and small deposits of bone called osteophytes or bone spurs may grow on the edges of the joint. Bits of bone or cartilage can break off and float inside the joint space causing pain and damage. A joint capsule is a tough membrane sac that encloses the articulating ends of bones. Synovium is a thin membrane inside the joint capsule that secretes synovial fluid. Synovial fluid is a fluid that lubricates the joint and keeps the cartilage smooth and healthy. Collagen is a family of fibrous proteins, which are the building blocks of skin, tendon, bone, and other connective tissues. Proteoglycans are made up of proteins and sugars that interweave with collagen and form a mesh-like tissue. Chondrocytes are found throughout the cartilage and are cells that produce cartilage and help it stay healthy as it grows. Ligaments, tendons, and muscles are tissues that surround the bones and joints and allow the joints to bend and move. Muscles are bundles of specialized cells that, when stimulated by nerves, either relaxes or contracts to produce movement. Those affected with osteoarthritis may have muscular atrophy due to decreased movement because of pain, regional muscle atrophy, and lax ligaments.
Generic 60 caps purim visa
Source: Connecticut Department of Public Health 9 treatment issues specific to prisons order line purim, Tuberculosis Cases at cases were among persons who were born outside of the a Glance, Connecticut, 2011. Acute hepatitis B is more 60 49 49 common among persons 25 to 44 years of age, males, 39 black non-Hispanics, persons who have had multiple sex 40 31 267 24 partners, and men who have sex with men. Between 2002 and 2011, the number of acute hepatitis B cases ranged from 102 cases in 2002 to 19 cases in 2011. Source: Connecticut Department of Public Health, Reported Chronic Hepatitis B, by Town, 2011. Prior to 1992 when widespread 10 screening of the blood supply began, Hepatitis C was also 0 2007 2008 2009 2010 2011 often spread through transfusions or transplant. Source: Connecticut Department of Public Health, Viral Hepatitis Surveillance Program, Acute Hepatitis C Cases by Year Reported, 2007 Disparities 2011. In 2011, the towns of Bridgeport, New Haven, Waterbury, New Britain, and Hartford had more than 60. Hispanic adults, respectively, reported getting the Source: Connecticut Behavioral Risk Factor Surveillance System, 2012. Over this same period, the number of pertussis or whooping cough cases ranged. The number of cases for other food-borne 0 and water-borne illnesses remained relatively steady 2006 2007 2008 2009 2010 2011 2012 over this period. Source: Connecticut Department of Public Health, Reported Cases of Over the 2003 to 2012 period, the annual number of Disease by County, 2006-2012. Of note, the number of rabies cases is not a measure of the overall 50 number of rabid animals in Connecticut, as animal testing 21 9 4 8 11 9 for rabies is conducted to help manage potential human 0 0 and domestic animal exposures. In 2012, there were 21 2006 2007 2008 2009 2010 2011 2012 cases of West Nile virus Source: Connecticut Department of Public Health, Reported Cases of Over the 2002 to 2012 period, bats, cats, dogs, raccoons, Disease by County, 2006-2012. Findings in Connecticut Over the 2002 to 2012 period, the incidence of new cases of Lyme disease was highest in the northeastern region of the Connecticut, as well as the eastern region. The number of West Nile Virus cases was highest in the southwestern region of Connecticut over the 2002 to 2012 period. Health care facilities, 15 particularly acute care facilities, are a major source of * 287 10 infection. Trends Source: Connecticut Department of Public Health, Active Bacterial Core Surveillance Program. Over the 2001 to 2012 period, there was a significant decline in overall rates of methicillin-resistant Table 14. Non-fatal falls among older 300 293 adults result in $19 billion in annual medical costs. In Connecticut from 2001 to 2010, motor vehicle accidents, falls, and accidental poisoning were the. The number of deaths due to falls nearly doubled (n=358) 89 between 2001 and 2010. Similarly, in 2010, the number 164 229 163 of deaths due to accidental poisoning was 1. Motor vehicle accidents Motor vehicle accidents Disparities Accidental poisoning & exposure to Accidental poisoning & exposure to Connecticut males are nearly twice as likely as females to noxious substances noxious substances die from unintentional injuries. Motor vehicle accidents, Falls Falls accidental poisoning, and falls were the top three causes Accidental drowning and Accidental drowning and of death for males in 2010. In contrast, falls were the submersion submersion primary cause of unintentional injury death for females, Exposure to uncontrolled fire in Exposure to uncontrolled fire in structure or building structure or building followed by accidental poisoning and motor vehicle Source: Connecticut Department of Public Health, Vital Statistics, 2010, accidents. The 100 increases in accidental poisoning mortality were highest among females, white non-Hispanics, and young people 295 15 to 24 years of age. From 2000 to 2009, deaths due 90 to accidental poisoning doubled for persons 15 to 19 296 81. Both sexes Males Females Findings in Connecticut Source: Connecticut Department of Public Health, Hospitalization Tables, Table H-1, 2011. The rates of hospitalizations due to 4000 3,710 3,529 poisoning were similar for males and females (78. Source: Connecticut Department of Public Health, Mortality sports-related injuries (100. The 80 Children in rear seat percent in child restraint seats ranged from 100% in 2007 75 to 84. The percent of children in the rear seat 2003 2004 2005 2006 2007 2008 2009 of the car ranged from 95. The observed seat belt use in Connecticut increased from 78% in 2001 to 88% in 2010. There were no differences in 80 unsafe driving behaviors among students by sex, race, or 75 ethnicity, but there were differences by age. The in western and eastern Connecticut due to small highest premature death rates occurred in many of the numbers of events, this map suggests that from 2006 to same towns. It is estimated that 200 Male Homicides suicides result in $3,056 in medical costs per person, and Male Suicides $815,963 in work loss costs per person, resulting in a 150 313 Female Suicides $26. In 2006 to 2010 (data not shown) rates of homicide deaths and premature deaths were significantly higher for black non-Hispanics and Hispanics, compared to white non-Hispanics. During the same period, rates of death and premature death for suicide were significantly higher for white non-Hispanics, compared to every other racial and ethnic group. Deaths due to homicide are All ages N/A highest among persons 15 to 34 years of age and males, <1 Yr Both sexes 315 1-4 Yrs N/A particularly black non-Hispanic males. There are also N/A Males disparities in deaths due to suicide, with a higher suicide 5-9 Yrs 316 10-14 Yrs Females rate among males as compared to females. Suicide patterns for 35-44 Yrs 45-54 Yrs males and females differ by age, with highest rates for 55-64 Yrs females 45 to 54 years of age, and for males 75 years and 65-74 Yrs 318 older. The homicide 20-24 Yrs 25-34 Yrs rate was highest for persons 20 to 24 years of age (12. In Connecticut, about two-thirds of all homicides and one-third of all suicides are committed with firearms. All races/ethnicities White non-Hispanic Black non-Hispanic Hispanic Source: Connecticut Department of Public Health, Mortality Tables, Age-Adjusted Mortality Rate by Race and Ethnicity, 2006-2010. Homicide Suicide From 2005 to 2009, the proportion of students who Note: All racial groups are non-Hispanic. N/A indicates data not reported that they attempted suicide was similar for available. In 2011, however, female students Tables, Age-Adjusted Mortality Rate by Race and Ethnicity, 2006-2010. Persons who Criminal experience domestic violence may experience lost work 320 mischief, 131 days, physical injury, mental trauma, and even death. Risk of injury, In addition, persons who witness domestic violence are Disorderly 114 at greater risk of perpetrating violent behavior than conduct, 321 Breach of 6,950 those who did not witness domestic violence. While peace, most cases are not reported to the police, nonfatal 4,214 domestic violence is greatest among females 20 to 24 322 Assault, years of age. The greatest proportions of 350 arrests associated with family violence were for 300 disorderly conduct, assault, and breach of peace. The estimated 8 lifetime cost of child maltreatment cases that are 325 reported in a single year is $124 billion. Hispanic 10 students were more likely than white non-Hispanic students to report ever being forced to have sexual 5 intercourse. Work and the workplace can affect health through exposures to adverse physical conditions, but 2 also can serve as a setting where employees can engage 1. While occupational 2 safety and health have improved over the last several 1 decades, work-related injuries, illnesses, and deaths 331 persist. It is estimated that non-fatal occupational 1 injury or illness results in at least one day of work loss cost of $745 per employed worker in Connecticut, or 0 332 $867 million. Fatal injuries cost the State of Connecticut an estimated Source: Bureau of Labor Statistics, Census of Fatal Occupational Injuries.