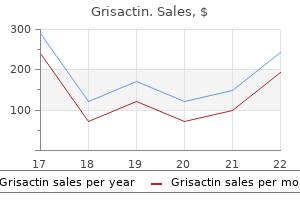
Grisactin
Buy grisactin now
An outline of the investigation protocol must be provided with specific mention of possible allergic reactions to intravenous contrast administered at abdominal imaging and the risks attached to a liver biopsy medicine cabinet buy discount grisactin line. However, donor confidentiality remains paramount and the reasons for declining a donor should not be volunteered to the recipient or other family members without explicit consent. A generic statement about the suitability of a donor with reference to the stringent assessment criteria can be helpful in providing an explanation. The donor should be informed of this ethical principle before assessment (see section 6). Enquiries about living donation originate predominantly from recipient family members, of whom a significant number will be unsuitable to be considered as donors. Emphasis is placed on the earliest possible identification of these inappropriate donors, given the intensive labour and cost resources of assessment. It is recommended that an initial telephone interview, followed up by a standardised triage questionnaire is completed by a senior transplant coordinator / specialist nurse. Potential contraindications to proceeding with assessment can be discussed within the multi-disciplinary team at an early stage. If the donor and recipient are not compatible, this provides an early opportunity to enquire about other potential donors. In most units, donor assessment at this stage will be arranged by a senior transplant coordinator / specialist nurse supported by a clinician. The clinician, normally a physician / hepatologist, undertakes the medical examination of the potential donor. To avoid conflict of interest, the donor clinician should not have direct responsibility for the care of the transplant recipient. A senior surgeon will take responsibility for both donor and recipient surgical safety. Additional support from radiology, cardiology, haematology and infectious disease colleagues may be necessary. Requirements include: determining the general medical health of the donor establishing the integrity of the donor liver function and potential graft quality assessing the risk of donor-derived transmission of disease to the recipient establishing the suitability of vascular and biliary anatomy psychosocial evaluation, including the capacity to give valid consent and the motivation for donation (see section 7). Best practice includes a standardised questionnaire and a pre-determined investigation order set. It is important to emphasise that the pace of the donor work up must be driven by donor safety and the provision of adequate time for informed consent, even when the potential recipient is very sick. Morbidity and mortality is disproportionately higher in older patients after hepatectomy, both in disease-generated and living-donor procedures. The medical evaluation, particularly of the cardiovascular system, needs to be especially rigorous in older donors. Formal testing to exclude occult ischaemia is recommended in donors of 45 years or over. Defining an upper age limit for liver donation is not feasible as other individual donor factors and the volume of the proposed liver resection required must be taken into account. There are specific considerations when assessing young mothers/female donors for donation: Pregnancy is a contraindication to donation Early counselling should be offered about non-pharmacological or progesterone-only contraception. Combined oestrogen and progestogen preparations should be avoided and/or stopped due to an increased risk of thrombosis. Peri-operative wound and urinary infection, venous thrombosis and cardiorespiratory events are more frequent. The frequent co-existence of obesity with the metabolic syndrome and fatty liver disease adds to complexity and risk. All overweight potential donors need careful evaluation of the liver parenchyma for macrosteatosis by imaging-based methodology, and potentially liver biopsy (see section 8. This is crucial as hepatic steatosis is a recognised risk factor for poor graft function; a recent systematic review showed an increased risk of poor graft outcome in livers with moderate-severe steatosis (6). Mild to moderate hypertension that is controlled with one or two antihypertensive agents is not a contraindication to donation providing significant end organ damage has been excluded. Consideration of patients with diabetes requires careful evaluation of the risks and benefits. In the absence of evidence of target organ damage and having ensured that other cardiovascular risk factors such as obesity, hypertension or hyperlipidaemia are optimally managed, diabetics can be considered for liver donation. Cardiovascular stress testing should be routinely performed in the majority of this patient group (see section 8. Cardiomyopathy, particularly hypertrophic cardiomyopathy (incidence 1:500), is the most common cause of sudden cardiac death in apparently healthy young people who would otherwise be ideal donors (7). The presence of overt cardiac disease will exclude most individuals as potential donors. In view of the relative risk associated with donor hepatectomy in comparison with donor nephrectomy, a lower age threshold of 45 years (which approximates to a 3-5% risk of coronary disease) is recommended. Coronary vessel calcium scoring appears to be the best discriminant investigation for coronary artery disease. Functional capacity can be assessed formally with a treadmill or more simply using the Duke Activity Status Index (a short questionnaire). Where there is uncertainty about functional capacity or identification of other risk factors, cardiology review is recommended. Investigation protocols are influenced by local service provision and access to the different modalities for assessment. It quantifies the functional capacity to respond to increased metabolic demands and generates a patient-specific measure of risk. The individual risk of thrombosis following surgery can be more accurately defined by characterising underlying genetic profiles and performing a thorough thrombophilia screen. An extensive panel of investigations (acquired and genetic risk factors) is recommended (see section 8. Prophylactic anticoagulation will be suitable for most low-risk candidates but will be absolutely contraindicated for certain profiles. Input from a haematologist with an interest in sickle cell disease is recommended. Thalassaemia Patients with thalassaemia (major, intermedia and haemoglobin H disease) are not suitable for living liver donation as their requirement for blood transfusions causes iron overload and associated liver damage. Haemoglobin C & Haemoglobin E these haemoglobinopathies may be seen in donors of non-northern European heritage. Neither should pose a problem to liver donation except where Hb C is combined with sickle haemoglobin i. Such patients behave like patients with sickle cell disease and therefore should not be considered. Red cell membrane disorders these disorders, including hereditary spherocytosis, hereditary elliptocytosis and inherited haemolytic anaemias may be acceptable in mild forms. Expert haematological review of donors presenting with these disorders is required. However, case reports of transplantation mediated alloimmune thrombocytopenia associated with the transfer of donor anti platelet alloantibodies do indicate a potential for harm, and careful risk assessment and counselling is indicated (16). A1) Imaging must assess fatty infiltration in addition to the biliary and vascular anatomy. The topics that need to be covered in the clinical history and laboratory screening tests for chronic liver disease have been listed previously. Imaging of the liver is performed to investigate for signs of chronic disease, the presence of portal hypertension, and fatty liver disease. The latter is a common finding and the level of steatosis influences donor and recipient outcomes after liver transplantation (see sections 9. As the level of steatosis increases from mild to moderate (30%) to severe (60%), the risk of graft dysfunction and renal failure in the recipient increases (6). Early mortality and the frequency of severe ischemia-reperfusion injury also increase significantly. For these reasons, imaging is performed to allow an estimation of fat quantification.
Anémone � Lobes Aigus (Liverwort). Grisactin.
- Liver diseases and liver conditions such as hepatitis, stomach and digestive discomfort, stimulating appetite, treating gallstones, regulating bowel function, stimulating the pancreas, high cholesterol, varicose veins, stimulating blood circulation, increasing heart blood supply, strengthening nerves, stimulating metabolism, menopausal symptoms, hemorrhoids, and other conditions.
- What is Liverwort?
- Are there safety concerns?
- How does Liverwort work?
- Dosing considerations for Liverwort.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96086
Discount 250mg grisactin with amex
Among (37) used epinephrine injection as well as bipolar coagu Crohn patients medications online purchase grisactin 250mg online, bleeding localization has been said to be lation. Two studies have contradicted this, ulcerative colitis endoscopically, using injection of a mix however. One cited the colon (6) and the other the ileo ture of absolute alcohol and 1% polidocanol. Hemor rhaging has been observed in colitis caused by Salmonella typhi, tack due to various causes. Pseudomembranous colitis can also manifest as acute lower gastrointestinal bleeding. Patchy ulceration on the Bauhin valve with small visible vessel on the ulcer pathogen detected. Diminished levels of short those requiring operative intervention are especially at risk. In a chain fatty acids in the colonic lumen, which nourish the mu study by Bini et al. The cause of radiation colitis is disrupted cellular proliferation and regeneration as well as induction of inflam Nonsteroidal anti-inflammatory drugs can also in matory processes in the colonic mucosa. Possibilities for endo duce colitis, which may not be visibly discernible scopic therapy are usually limited. Nonsteroidal also include flat and usually irregularly bordered erosions anti-inflammatory drugs can promote bleeding from any num and ulcerations, which are surrounded by an otherwise nor mal appearing mucosa ( 13. In the right hemicolon, in contrast, they do not manifest with rectal bleeding until after they are clearly ulcerated. Based on our experience, injection therapy and me means of noncontact thermocoagulation. Thermocoagulation using contact methods is less sui gastrointestinal bleeding from benign polyps is poly table because tearing of tissue after completing coagula pectomy ( 13. In circumscribed bleeding sources, especially with vis ible vessels, mechanical methods such as hemoclipping can also be used. Therapy with hemoclips seems to be the more reliable method based on our own experience in that they Generally, it is larger polyps with a diameter greater guarantee mechanical closure of the vessel if applied than 1 cm that bleed (Fig. The most common cause of lower 135 i Acute and Chronic Lower Gastrointestinal Bleeding 13. Visible vessel can be seen after irri gation (b) at the base of the resection wound. Bleeding was definitively controlled by application of three hemoclips (Olympus) (c). The visible vessel on the edge of the resection site was closed with two hemoclips (Olympus) (g). Not infrequently, the cause of rebleeding lies in anticoagu Anorectal causes of acute lower gastrointestinal bleeding can be lant use, which is resumed too soon or not discontinued before detected in fewer than 10% of patients, whereby hemorrhoids the biopsy. The exact prevalence is difficult to determine, as some studies of acute lower gastrointestinal bleeding do not include anorectal causes. A visible vessel can be seen on the upper edge of the resection defect (a), which led to massive rebleeding. An additional clip is used to definitively compress and close the visible vessel (c). The mucosa is slightly elevated around the bi opsy site as a result of submucosal bleeding. In recent years, however, endo scopic alternatives have established themselves in the Anal fissures. The patient typically has has proved an especially effective and easy-to-learn severe pain upon spreading the anus, but the lesion can be care method for treating internal hemorrhoid bleeding. Bleeding from fissures usually ceases spon heater probe therapies of bleeding internal hemorrhoids. A bloodsoaked polypoid form is visible with a slight ring around the base where it was ligated (a). Following removal of the elevated tissue, hemorrhagic oozing ensued (b), and bleeding was stopped mechanically using three hemoclips (Olympus) (c). Heavy susception (internal rectal prolapse) causes excessive straining bleeding is rare. The lesion controlled using hemoclips and did not stop healed with conservative therapy and without until after injection of acrylic glue. Postoperative rectal bleeding There are no comparative studies on optimal endoscopic (Fig. Hemoclips can be applied or local injection of cosa has been damaged by prior radiation therapy. A case of polypoid cavernous hemangioma of the sig moid colon excised by colonoscopic polypectomy. Amer tal manipulation on the part of the patient can cause quite seri ican Society for Gastrointestinal Endoscopy. The role of endoscopy in the patient with lower gastrointesti nal bleeding: Guidelines for clinical application. Angiodysplasia of the right colon: a cause of gastroin Rectal bleeding following diagnostic procedures such as testinal bleeding. Determination of the optimal technique for bipolar electro ease: characteristics of a unique series of 34 patients. Acute major gastrointestinal hemorrhage in inflam scopic appearance of normal colon vasculature and colon vascular matory bowel disease. Frank rectal bleeding: a prospective study of causes logic spectrum of nonsteroidal anti-inflammatory drug-induced le in patients over the age of 40. Natural history and efficacy of ther scopic method: comparing the hemostatic efficacy of mechanical apeutic interventions. The argon plasma coagulator: a new and and management of lower gastrointestinal hemorrhage. An annotated algorithmic approach to acute lower Clin Biol 1999;23:A54 (Abstract). Early predictors of severity in acute matory drugs risk factors for hemorrhage and can colonoscopy pre lower intestinal tract bleeding. Stigmata associated with recurrence of lower hospital stay in patients with acute lower intestinal bleeding. Argon laser therapy for hemorrhagic by endoscopic injection of absolute ethanol and 1% polidocanol. Management of the adult patient with acute lower clinical presentation and diagnosis. Angiodysplasia is defined as a di with hollow areas lined with en lation of superficial vessels while hemangiomas are defined as dothelium (courtesy benign vascular tumors. Wagner, the difference between the two is merely gradual and whether Institute for differentiation reflects differing pathogenesis remains unan Pathology, Augsburg swered. Angiodysplasia (Telangiectasia) Epidemiology and Pathogenesis the pathogenesis of angiodysplasia is not entirely clear.
Buy grisactin visa
The method of ductal access as well as specific issues of papillary cannulation should be noted symptoms of breast cancer generic grisactin 250 mg mastercard, to acknowledge an increased risk of pancreatitis or other com plications. Measurements should be presented in millimeters or centimeters insofar as possible. Therapeutic measures should be described in detail, for example, caliber of dilating catheters, length and size of balloons and stents, duration of dilation procedures. In-procedure unplanned events should be described, with measures taken to remedy the situation, and the outcome at the end of the procedure. It should also be stated whether the event changed the outcome or results of the procedure per se. Recommendations should be made as to immediate monitoring, but also about the interpretation of findings, repeat procedures, or other fol low-up. Easily accessed storage of endoscopic images has been scarce, partially due to lack of suitable hardware, difficulties to integrate medical record systems in general, and also because of the focus on the X-ray images. The radiology images tend to live in the world of radiology, with separate protocols, hardware, and storage mechanisms and even networks. Reading and reporting the X-ray images, often suboptimally captured by the endoscopist, is difficult for radiologists who are usually not present during the procedure [7, 8]. This is unfortunate, and it would be good to strive for a more joint documentation mechanism in the future. Making sure that the radiologist receives a copy of the endoscopy report is essential. Hopefully, integrated electronic medical record systems may remedy this dysfunctional dualism. However, some general principles can help to optimize the quality (and quantity) of radiographic imaging [8]. This should be a part of your compulsory start-up routine together with checking all of the equipment and X-ray shielding. Usually, a direct anteroposterior angle is preferable, although other angulation may occasionally be useful. This is particularly important in the unlikely event of adverse events, for example, perforations. Make sure any foreign bodies (cables, cloth details, piercings) are removed from the field of interest. Without this, calcifications in ribs or vessels, and recent contrast imaging, may cause much confusion. Frequently, these first images with limited contrast saturation are the most instructive, particularly to delineate hilar anatomy or reveal the location of leaks. This may require balloon occlusion, in particular in the setting of narrow or obstructed intrahepatic ducts, to avoid preferential overfilling of the gallbladder or contrast leak through a papillotomy. Angulation of the imaging or temporary repositioning of the endoscope may be necessary to capture the key elements. Emptying dynamics of the intraductal contrast may be important, and sometimes additional imaging in the supine position may add useful extra information, particularly in terms of better right-sided filling. However, any pathology or aberrations should be captured, for example, a duodenal ulcer, suspected invasive cancer, strictures or periampullary diverticula, or any pathological appearance of the ampulla. However, therapeutic procedures are often better conveyed with video, and the utility of video storage is likely to 212 Chapter 13 increase in the future as this format is more easily transferred across networks and computer systems. In lesions deemed nonresectable by endoscopy the imaging is important to the sur geon (or for the palliative strategy as a starting point). The most important of these are delayed adverse events, outcomes of already recorded intraprocedural events, and pathology reports. With a broader perspective, out comes of the procedure are also of interest, but this information may be better traced in the context of the general medical record system. While intraprocedure events are a natural component of the endoscopy report, delayed events are a more difficult issue. While the responsible endoscopist may indeed be to blame, the adverse events reporting must be done independently of this aspect. Ideally, the endoscopy report should be updated when the pathology reading is ready, and some software systems allow this. If not, the general medical record system must somehow cater for linking the two, and any resulting new diagnoses and recommendations. For immediate use, a report format for the recovery room personnel would be of importance, perhaps more formatted for anesthesiolo gists in the context of deep sedation or general anesthesia, where extended monitoring is warranted. Some endoscopists give them a copy of the report going to the referring physi cian, but a more focused version is preferable. This should include the important findings and conclusions, but in layman terms, and probably with somewhat more elaborate explanations and perhaps some pertinent sketch drawings. The report might also preferably include or be combined with pertinent disease descriptions, more elaborate anatomical explanations, or links to additional reading material on the Internet. Finally, cumulated reports are needed for other purposes, for example, quality assurance programs, financial purposes, or hospital statistics. Thus, the output information is no longer strictly linked to what information is entered, and diverse reader categories can be addressed more to the point. Cumulative, or at least anonymized, data may also be fed into joint data repositories for multicenter quality assurance purposes. Increasingly, however, the diverse needs for documen tation noted earlier call for dedicated databases that will generate the appropriate reports. A number of such systems are commercially available, variably integrated in hospital-wide databases. The main challenge of the software vendors is to develop an interface that presents the required structure of the database in a format that is acceptable for the user. There is a natural conflict between necessary structure on one side and the endoscopist need for flexibility and natural language on the other. Unless this dilemma is solved, the quality of the structured input data will suffer, and the data collected will not accurately convey the reality of the endoscopic activity. The structure standards presently being recommended may offer an important input for the software companies. The recommendations for terms, attributes, and components of the endoscopy report should form at least default templates 214 Chapter 13 for the various software solutions. While these may obviously be amended or expanded, such a common platform still presents a joint basis that will help standardize endoscopic reporting throughout the world. Working Party Report by the Committee for Minimal Standards of Terminology and Documentation in Digestive Endoscopy of the European Society of Gastrointestinal Endoscopy. Image documentation of endoscopic findings in ulcerative colitis: photographs or video clips Postprocedural interpretation of endoscopic retrograde cholangiopancreatography by radiology. It results from bile duct obstruction and subsequent bacterial superinfection of the stagnant bile [1]. Pain may be transient or mild, and jaundice may be mild if the ductal obstruction is of recent onset or incomplete. This condition carries a significant risk of rapid deterioration and mortality, requiring aggressive resusci tative measures (fluid, broad-spectrum antibiotic, and intensive care) and urgent drainage of the obstructed and infected bile duct [2]. An indwelling biliary stent predisposes to bacterobilia, and blockage of the stent often leads to acute cholangitis. Similarly, a previous sphinc terotomy causes duodenobiliary reflux and bacterobilia and may lead to cholan gitis or stone recurrence [4]. Because of protection from the flushing effect of normal bile flow and the anti bacterial effects of bile salts and biliary IgA, bacterobilia alone does not necessarily cause acute cholangitis [5]. However, in cases of biliary obstruction, the resultant reduced bile flow and impaired Kupffer cell function lead to acute cholangitis [6, 7].
Buy grisactin 250mg mastercard
Chapter 7 / Infectious Diseases 389 What is the antimicrobial Streptococci treatment tinnitus order grisactin cheap online, methicillin-sensitive spectrum of rst-generation Staphylococcus aureus, some community cephalosporins What is the antimicrobial Expanded activity against gram-negative spectrum of third rods. Ceftazidime has even less activity against gram-positive cocci but is an excellent antipseudomonal agent. What is the antimicrobial the rst fourth-generation cephalosporin spectrum of fourth is cefepime. What is the antimicrobial Most gram-positive and gram-negative spectrum of the aerobic and anaerobic pathogens carbapenems (imipenem except for Burkholderia cepacia, and meropenem) What is the antimicrobial Activity against aerobic gram-negative rods spectrum of aztreonam What is the antimicrobial Aerobic and facultative gram-negative spectrum of aminoglycosides How can aminoglycoside Careful monitoring of blood levels, serial toxicity be avoided Rocky Mountain spotted fever, ehrlichiosis, and Chlamydia infections; Borrelia burgdorferi and Mycoplasma sp. What are the major Discoloration of teeth and bones in toxicities of tetracyclines Chapter 7 / Infectious Diseases 391 What toxicities are Reversible bone marrow depression in associated with adults receiving 4 g or more per day and chloramphenicol As 1 of several agents for mycobacterial infections As part of combination therapy with erythromycin in severely ill patients with legionellosis Occasionally as combination therapy for severe gram-positive infections What is the antimicrobial Anaerobes (strict anaerobes), although spectrum of metronidazole Erythromycin, clarithromycin, and azithromycin What is the antimicrobial Most gram-positive pathogens (including spectrum of erythromycin Streptococcus pneumoniae [although resistance is rapidly increasing], Strepto coccus pyogenes, and Corynebacterium diphtheriae), Bordetella pertussis, Legionella pneumophila, Mycoplasma sp. There is resistance in up to 50% of gram-positive organisms, thus limiting the role of this agent in empiric treatment of respiratory tract infections. What is the antimicrobial Aerobic gram-negative rods; Haemophilus activity of older quinolones sp. These quinolones are not the therapy of choice for infections caused by staphylococci and streptococci. Chapter 7 / Infectious Diseases 393 What is the antimicrobial Enhanced gram-positive activity and activity of newer quinolones therefore indicated for empiric respiratory. What is the antimicrobial Speci c gram-negative rods only, including activity of colistin What are the major adverse Ototoxicity (particularly vestibular distur effects of streptomycin Possible hepatotoxic drugs are reintroduced 1 at a time to identify the offending agent. What are the second-line Capreomycin, kanamycin, amikacin, antimycobacterial agents Cryptococcus neoformans), dimorphic fungi (including Blastomyces dermatitidis, Histoplasma capsulatum, Coccidioides sp. Chapter 7 / Infectious Diseases 395 How are acute reactions to Premedication with acetaminophen, amphotericin minimized What are the advantages Similar ef cacy with less renal toxicity and disadvantages of but at a considerably higher dollar cost, lipid-encapsulated and some forms do not cross into the amphotericin B What is the antimicrobial In vitro and in vivo activity has been spectrum of voriconazole What is the indication for Invasive Aspergillus infections, the use of voriconazole What is the antimicrobial Most candida species as well as molds spectrum of posaconazole If treatment is begun within 24 hours after a varicella zoster rash rst appears, it decreases the severity of varicella in children and adults. If begun within 2 days of the onset of illness, they may decrease the duration of symptoms. What are the uses of the Also available for treatment of in uenza A other neuraminidase and, unlike rimantadine and amantadine, inhibitors, oseltamivir and also active against in uenza B zanamivir What are the common side Renal toxicity, which is usually reversible effects of foscarnet Unicellular organisms (prokaryotes) What is the difference Structural differences in the cell wall of between gram-positive and bacteria, so the staining properties on gram-negative bacteria Gram staining are different How can bacteria be further As aerobes or anaerobes classi ed What are the common organisms and the common syndromes that go with each of the following: Organism: Gram-positive cocci Staphylococci (S. Diarrhea, skin and soft-tissue infections, bacteremia Gardnerella Bacterial vaginosis, endometritis Haemophilus spp. Bacteroides, Prevotella, and Fusobacterium How do anaerobic infections Anaerobes gain access to usually sterile occur What are the spirochetes Treponema pallidum (syphilis), Leptospira, and their associated Borrelia (Lyme disease, relapsing fever), diseases They produce multisystem general diseases that they disease, with most organisms producing a cause Zoster results from reactiva tion of latent virus in dorsal root ganglia; it does not require new contact. Bacterial superinfection of lesions, encephalitis, cerebellar ataxia, and pneumonitis. Chapter 7 / Infectious DiseasesChapter 6 / Hematology 403403 How can Ramsay-Hunt Immunocompromised patients exposed syndrome be prevented Varicella vaccine is available and indicated in nonimmune children older than 12 months and in adults. What is the time course or use for the following virus speci c antibodies: Viral capsid antigens Occur early in disease and are seen at presentation in 80% of cases IgM antibodies Persist for a lifetime Chapter 7 / Infectious DiseasesChapter 6 / HematologyChapter 6 / HematologyChapter 6 / HematologyChapter 6 / HematologyChapter 6 / Hematology 405405405405405405 Early antigens and these antibodies remain positive for life Epstein-Barr nuclear and are not helpful in diagnosing acute antigen What are the clinical Plantar warts, at and common warts, manifestations of anogenital warts (certain types of papillo papillomaviruses What is the treatment for Most therapies involve physical or papillomavirus infection A nonspeci c festations of mumps virus prodrome is followed by earache and infection Meningitis occurs in up to 10% of patients with parotitis, but only 50% of patients with mumps meningitis have parotitis. Epididy moorchitis is the most common nding in adult men, occurring in 20% of men with mumps.
Cheap 250 mg grisactin with mastercard
Rapid assessment is required to rule out History bacterial infection treatment alternatives for safe communities discount 250mg grisactin with amex, which qUickly leads to irreversible joint damage if not treated. Accurate diagnosis Duration of symptoms assists in diferentiating the requires joint aspiration and examination of synovial cause of joint inflammation. These diseases are discussed in detail in However, gout and rheumatologic disease may also Chapters 57, 58, and 59. They hegin as small papules and then Count quickly become pustular with a necrotic center. Other fndings to look for on (rheumatologic, crystalline) skin examination include gouty tophi (subcutaneous nodules found on extensor surfaces), needle track 50, 000-100, 000 Severe inflammation (sepsis or gout) marks (risk for septic arthritis), and psoriatic plaques (spondyloarthropathy). Gout primarily exclude infection, because damaged joints are more affects the frst metatarsal joint or ankle joint but susceptible to infection. The presence of osteoarthritis may be noted, Septic arthritis has a predilection for damaged joints; but this does not rule out other causes, such as therefore, joint aspiration still needs to be performed crystalline disease or infection. Lyme antibody cannot distinguish graphic guidance and should be performed by a between active and inactive infection, but a negative specialist. Gout often occurs in the frst metatarsal or ankle nonsteroidal anti-inflammatory drug such as joint. Weakness of dorsifexion occurs in L5 root Patients older than 50 or those with a history compression, and weakness of plantar flexion occurs of weight loss, signifcant trauma, malignancy, or in S] root compression. A positive sign reproduces sciatica at 30 to 60 ibuprofen or naproxen degrees of elevation. Bone scans are useful when searching for nancy should receive an initial lumbar spine flm; osteomyelitis or malignancy when plain flms are magnetic resonance imaging should be reserved unrevealing. Joint aspiration is usually performed to rule out other causes, such as infection or gout. Alcohol however, and fa lse positives occur in the elderly should certainly be avoided because it greatly and in patients with other autoimmune diseases, increases risk of liver damage. Psoriasis is characterized by erythematous scaly lesions, usually seen on extensor Hand flms in advanced psoriatic arthritis may reveal surfaces of the extremities, and nails may show erosion of the distal interphalangeal joint, giving a pitting or onycholysis.
Best order grisactin
The best opportunity to discover malignancy within a simple cyst is by careful inspection of the cyst wall at open surgery 6mp medications buy grisactin australia. The risk of malignancy in a simple biliary cyst is small, but eight cases of adenocarcinoma and five cases of squamous cell carcinoma have been reported. While this may be more frequent in situations where the cyst was managed without histologic evaluation, it may also occur where the initial histology showed a flat cuboidal epithelium without papillary projections. Laparoscopic surgical treatment Laparoscopic management of the hepatic cysts is emerging as a new, less invasive therapeutic option. This procedure, as in open surgery, involves wide unroofing of all non-parenchymal cyst wall to allow fluid produced from the epithelial cells of the cyst wall to drain into the free peritoneal cavity where it can be absorbed, as shown in Fig. They can be cauterized and sutured38 or, alternatively, the endoscopic vascular stapler can be used to resect the cyst wall. This technique is perhaps technically easier and faster than intracorporeal suturing and secures blood vessels and bile ducts effectively. The creation of a flap of omentum off the transverse colon to pack in the cyst cavity may decrease the risk of recurrence. The gallbladder should be removed if it contains stones or is adjacent to the cyst wall being resected. The rationale for cholecystectomy is to prevent the need for reoperation in a scarred area and eliminate the risk of torsion of a free-floating gallbladder. Furthermore, a symptomatic gallstone can produce pain that is indistinguishable from hepatic cystic disease. An intraoperative cholangiogram is useful in identifying any connection with the biliary tree, which can then be oversewn. The selection of patients with symptomatic hepatic cysts for laparoscopic treatment is important. Watson and Jamieson have reported successful treatment of a patient with a posterolateral cyst by placing the patient in the lateral position to gain access to the cyst wall. This problem may be partly resolved by the use of laparoscopic ultrasound to image the cyst wall. Nevertheless, symptomatic recurrence can occur and complication rates of around 10% are reported. Management strategies for benign cysts and polycystic Disease of the liver 313 Management of polycystic liver disease Most frequently multiple cysts in the liver present with a variable number of very large cysts (in general from one to five) associated with much smaller cysts. In the patients with isolated symptomatic large cysts symptoms are comparable to the patients with simple biliary cysts. The treatment consists of treating each one of these voluminous cysts the same as for the isolated simple biliary cysts. The treatment of deep small cysts is often ineffective: alcoholization of each of these cysts is possible but surgical fenestration is simpler and more adaptable. It is generally reported as successful in relieving symptoms, but is associated with a significant postoperative morbidity of around 50%. The situation is different when all the liver is occupied by multiple small cysts, because it is not possible on the preoperative examination to identify which of the cysts are responsible for the symptoms. The symptomatology of these patients is very different and is associated with painful abdominal distention, early satiety associated with vomiting, loss of muscle bulk and sometimes profound malnutrition. This intervention is long because it is necessary to fenestrate the deep cysts pocket by pocket by traversing the more superficial cysts. It must be done very delicately because the vasculobiliary structures are distorted between the cystic layers. It is almost always followed by ascites that can be prolonged and must be accompanied by a rigorous fluid and electrolyte replacement that can attain several liters. Surgical fenestration of polycystic liver disease is efficacious in about 75% of patients over the short term; it is accompanied by parenchymal hypertrophy in the remaining liver. Failures are observed in patients where there is no zone of non-cystic hepatic parenchyma and/or a very active cyst secretory epithelium. In the past, several authors have reported success with the fenestration/resection surgical approach. This is particularly useful when the cyst distribution is asymmetrical, as shown in Fig. Proponents of resection/fenestration report very adequate reduction of liver volume and prolonged relief of symptoms. Anatomy is always very distorted with intrahepatic and extrahepatic bile ducts and blood vessels Surgical Management of hepatobiliary and pancreatic disorders 314 Figure 11. While control of the hepatic pedicle with a Pringle maneuver is usually possible, control of the hepatic veins from above may be impossible because of intervening liver and cyst tissue. Because of difficulty with exposure once hemorrhage begins it may be very hard to control. With the absence of landmarks there is also the ever present danger of occluding the remaining hepatic vein, creating the acute Budd-Chiari Syndrome. Collapse of as many superficial liver cysts as possible before the resection is started may aid in exposure. The advantage is more prolonged relief of symptoms with the reduction of cyst surface area and less difficulty with postoperative ascites. These patients may benefit from a laparoscopic unroofing with omental interpositions, as in patients with solitary cysts. This minimally invasive approach offers immediate relief of symptoms and is probably Management strategies for benign cysts and polycystic Disease of the liver 315 associated with the least postinterventional problems. Patients that have a single dominant cyst that can be accessed by percutaneous needle insertion may also benefit from alcohol sclerotherapy. This approach is particularly attractive in elderly patients with co-morbidities, where surgical intervention may be hazardous. Fenestration has the advantage of being perhaps a less aggressive and easier approach. The risk of massive intraoperative hemorrhage may be less than with resection, and if the cyst walls are thin there is a satisfactory reduction in size that can result in prolonged relief of symptoms. Furthermore, extensive fenestration without resection exposes large amounts of a secretory biliary type of endothelium to the free peritoneal surface. Here no part of the liver is spared from involvement and the cysts are small, making fenestration difficult. Furthermore, the liver is often quite rigid, with significant fibrosis of cyst walls, limiting the amount of collapse that occurs with fenestration. Turnage reported significant morbidity and postoperative death in three out of five patients with this type of polycystic liver disease treated with resection and/or fenestration. Many of these patients present late or after a series of partially successful fenestration operations. Renal failure and a need for kidney transplantation may also prompt the decision to transplant the liver, using the same donor for both organs. Clearly, patients that are presenting late after previous surgical interventions, with massively enlarged livers and/or chronic renal insufficiency, should be treated differently from the patient presenting for the first time with pressure symptoms from a large dominant cyst. Prevention and management of biliary complications Biliary complications are among the most frequent postoperative problems. They most commonly present in the early postoperative period with a bile leak and/or biliary ascites. These leaks no doubt result from an inability to secure small bile ducts in the resected cyst walls. They also appear to occur with equal incidence with fenestration and fenestration/resection procedures. Leakage can be assessed intraoperatively by applying dry sponges on the raw areas and looking for bile staining, or by performing an intraoperative cholangiogram after cholecystectomy (a recommended procedure in all cases). Very small leaks may not be discovered on cholangiogram so injecting air or a dilute solution of methylene blue into the bile duct with direct vision of the resected area may be efficacious. Sewing a piece of bowel to a cyst creates a large, contaminated, Management strategies for benign cysts and polycystic Disease of the liver 317 poorly drained cavity that connects with the biliary tree.
Syndromes
- Wide pupils
- A carbuncle is located on the face or spine
- Stay up-to-date with immunizations
- Install railings or use aids such as a cane or walker to help prevent falls.
- Slowly resume activity. You may need help walking when you lose your balance during attacks.
- Herniation
- Rough places on dentures, fillings, and crowns
- Fever
Cheap 250mg grisactin free shipping
There is no evidence to suggest that infants with chlamydial infections should be isolated medicine vs medication purchase on line grisactin. Note that successful treatment of the mother during preg nancy with oral erythromycin or azithromycin prevents most cases of vertical transmission. Perinatal morbidity and mortality associated with chlamydial infection: a meta-analysis study. Chlamydia culture of the conjunctiva (for conjunctivitis) or nasopharynx (for pneumonia) remains the gold standard for diagnosis. However, cultures have many disadvantages; specimens require special handling, which can make transport to the laboratory challenging and generally require 3 to 7 days for processing, which may delay treatment. Sero logic diagnosis of chlamydial infections are diffcult to interpret and only done in a few clinical laboratories 109. Mothers with positive endocervical cultures should be treated during pregnancy to prevent vertical transmission. Chlamydia infection in both male and female genital tracts can be asymptomatic, which is why routine screening in pregnancy is warranted. However, the effcacy of prophylactic treatment is unknown; moreover, reports of an association between the use of oral erythromycin for pertussis and infantile hypertrophic pyloric stenosis have appeared. Neonates with chlamydial conjunctivitis or pneumonia should receive oral erythromycin base or ethylsuccinate, 50 mg/kg/day in four divided doses, for 14 days. The effcacy of erythromycin is approximately 80%; therefore a second course may be required, and follow-up of infants is recom mended. Limited data on azithromycin for treatment of chlamydial infection in infants suggest that dosing of 20 mg/kg as a single dose for 3 days may be effective. Its shorter treatment course and less severe gastrointestinal side effects could improve treatment compliance. Expi ratory wheezing occurs in fewer than 25% of infants with the disease; 60% have abnormal eardrum fndings. Although a severe illness is relatively rare, affected infants appear irritable, eat poorly, and cough often. The chest x-ray shows hyperinfation of the lungs with bilateral diffuse nonspecifc infltrates. Pos sible laboratory fndings include a distinctive peripheral eosinophilia (>300 to 400/mm3), mild arterial hypoxemia, and elevated serum immunoglobulins. Treatment of any previous conjunctivitis with oral erythromycin seems to prevent pneumonia, although there are case reports of treatment failures. Approximately 50% of the infants with chlamydial pneumonia do not have a history of previ ous conjunctivitis. Early-life chlamydial lung infection enhances allergic airways disease through age-dependent differences in immunopathology. Because most cases of neonatal osteomyelitis arise as a consequence of bacteremia, the organisms responsible for causing osteomyelitis refect the changing trends in the ethology of neonatal sepsis as well as the different likelihood of osteoarticular shedding within pathogens. Although osteomyelitis was rare in the past, recent studies suggest that it might be increasing in neonates. The overall rate of nosocomial bone and joint infections is approximately 1 or 2 in 1000 admissions. Hematogenous dissemination is responsible for most cases; however, skeletal infections can also result from the following: n Extension from infection in surrounding tissues. What distinct anatomic and physiologic features place the newborn infant at risk for osteomyelitis and septic arthritis Hematogenous infection of long bones is initiated in dilated capillary loops of the metaphysis, adjacent to the cartilaginous growth plate (physis), where blood fow slows, providing pathogenic bacteria with an ideal environment to multiply. In neonates there is an anatomic communication between the circu latory systems of the metaphysis and epiphysis (transphyseal vessels) that can lead to severe damage of the cartilage cells on the epiphyseal side of the growth plate when infection occurs. The vascular connection is obliter ated at 8 to 18 months of age when the epiphyseal and metaphyseal become totally separated. Decompression of the primary metaphyseal abscess through the adjacent cortex also permits entrance of pus into the articular space of the bones whose metaphyses lie within the articular capsule of the joint. Suppurative arthritis of hips, shoulders, elbows, and knees is frequently seen in osteomyelitis of the humerus or the femur (Fig. Why do neonates not exhibit many of the features of chronic osteomyelitis seen in older children and adults On account of a relatively thin cortex, the abscess usually spreads into the subperiosteal space and rapidly involves the entire circumference and length of the bone. This free communication between the original site of osteomyelitis and the subperiosteal space prevents the necrosis and cortical sequestra that happens in older children and adults. The effcient vasculature and fertility of the inner layer of the periosteum encourage early development of new bone formation (involucrum), permitting remodeling of bone within a very short time after the infectious process has been controlled. How often are bacterial culture results positive in neonatalosteomyelitis and septic arthritis Some studies report that approximately 17% of septic arthritis in premature infants is caused by Candida species. What is the frst line of management for a suspected septic arthritis in a newborn infant Joint aspiration with incision and drainage is appropriate whenever there is a signifcant collection of pus in the soft tissues. Often, surgical drainage is indicated for relief of intraarticular pressure when the hip or shoulder is affected. Neonatal osteomyelitis of the maxilla is a distinct clinical entity usually caused by S. The clini cal course of this condition begins with acute onset of fever and nonspecifc systemic symptoms that shortly after are accompanied by the following: n Early edema and redness of the cheeks n Unilateral nasal discharge n Swelling of the eyelid with conjunctivitis this entity can be confused with orbital cellulitis or dacryocystitis. Once cultures are obtained, the initial choice of antimicrobial agents must be based on the presumptive bacteriologic diagnosis. Osteomyelitis caused by enteric organ isms is suffciently common in neonates to justify adding an aminoglycoside to the initial regimen. If the organism is identifed and antibiotic sensitivities have been determined, treatment should be changed to the safest and most effective drug. In the neonatal age group, orally administered antibiotics are not used because there are insuffcient data regarding their absorption and effcacy. Males are affected more often than females in the neonatal period, and uncircumcised males are even more susceptible, with a threefold to sevenfold increased risk. Unlike in older infants, hematogenous spread of infection is more common in neonates than ascend lucencies, and periosteal elevation). Anatomic or physiologic abnormalities of the urinary tract, such as obstructive uropathy, Multiple sites of involvement can insensitive to the destruction of are also common underlying factors. Gallium bone In equivocal Tc bone scans, gallium the radiation scan dose is signifcantly the defnitive diagnosis is made by positive culture of urine that is obtained by percutaneus aspira might be useful. Urine from bags and other nonsterile materials should Sonography Most useful as a tool for guiding needle An experienced sonographer is not be used because false-positive results are very common. The yield of urine culture in neonates aspiration of fuid collections in joints or required. Urinalysis is not very helpful insofar as neither the presence nor absence of pyuria is completely It is inexpensive. However, an enhanced urinalysis (leukocytes measured in There is no radiation exposure. Other organisms include bone destruction, periosteal reaction and diseases (not however involvement of Proteus, Pseudomonas, Klebsiella, and Enterococcus species or S. The clinician should try to obtain a urine culture before initiating antibiotic treatment abnormal physical fndings. Laboratory data include the following levels: and then modify the treatment once culture results and sensitivities are known. The transition to an oral regimen depends on the clinical and the signs and symptoms suggest an acute infectious process. The urinalysis is consistent with a microbiological response and the presence of bacteremia or anatomic abnormalities. A second diagnosis of acute pyelonephritis (assuming that the specimen has been properly obtained). Unlike the distinction of cystitis and pyelonephritis in older infants and children, In the past, prophylactic antibiotics were often used for structural anomalies of the urinary tract or infection of the urinary tract in the neonate often involves the kidney.
Safe grisactin 250mg
Natural methods can support the body in overcoming an infection of the tonsils without the need for surgery treatment improvement protocol discount grisactin 250 mg with mastercard. The need for surgical intervention is indicated only in certain extreme situations. Most people believe that removing an inflamed appendix is a necessity and that diagnosing appendicitis is routine and reliable. But surgeons get it wrong up to 45 percent of the time, even when they perform an exploratory laporotomy in order to come up with a diagnosis. One in five patients with appendicitis leave the hospital without a correct diagnosis ever being made, and one in five appendixes removed by surgery is found to be normal. In addition, the mortality rate among patients with low risk heart disease who undergo a bypass operation is higher than it is among those with a high risk. A 1998 study, published by the New England Journal of Medicine, showed that patients who suffer a mild heart attack and are given a bypass or balloon angioplasty are more likely to die as a result of the surgery. Another study that involved researchers from 14 major heart hospitals around the world, found that up to one-third of all bypass operations were not only unnecessary, but actually hastened the death of the patient. Angioplasty, a relatively new procedure used to open arteries, offers an even lower survival rate than bypass surgery. The relief of chest pain (angina) that patients may experience after a bypass operation cannot always be attributed to an actual improvement of the condition. In the case of a bypass operation, the newly inserted pieces of coronary arteries can block up easily again if the cause of arteriosclerosis is not removed. Major lasting improvements were attributed to an improved diet and lifestyle, stress reduction, smoking cessation and regular exercise. Stents can also rescue someone in the midst of a heart attack by obliterating an obstruction and keeping the closed artery open, at least for a while. But as it turns out, the vast majority of heart attacks do not originate with obstructions that narrow arteries. Heart researchers now know that most heart attacks do not occur because an artery is narrowed by plaque. Instead, they say, heart attacks occur when an area of plaque bursts, a clot forms over the area and blood flow is abruptly blocked. They assert that in 75 to 80 percent of cases, the plaque that erupts was not obstructing an artery and would not have been stented or bypassed. Because the plaque which is attached to the artery walls is soft and fragile, it produces no symptoms and would not be seen as an obstruction to blood flow. True blockages in an artery would make themselves known as severe chest pain and breathing difficulties. Since heart patients may have hundreds of vulnerable plaques, surgeons cannot go after all of them. In fact, coronary artery surgery does nothing to the soft plaque, which is the real time bomb ticking in the coronaries of heart disease patients. According to a New England Journal of Medicine report, 1, 500 patients a year in the U. Wayward clamps, sponges, electrodes, retractors and various other instruments take up permanent residence in the chest, abdomen, hips and body cavities like the vagina. According to these findings, the chances of having such items planted in your body are higher if you happen to be overweight. Complications from these blunders can lead to internal bleeding, infection and sometimes death. In quite a few patients, though, these missing items are not discovered until the person undergoes another procedure or has an X-ray or ultrasound. Fear-Motivated Operations In the United States alone nearly one million women a year sacrifice their uterus to the scalpel. This means that more than half of all American women will have had a hysterectomy by the time they reach the age of 65. Many of these women will suffer from post-operative syndromes such as depression, anxiety and increased susceptibility to stress. I have seen in my own practice that most women who have had a hysterectomy developed ovary problems, breast lumps, digestive disorders or breast cancer 1-5 years after the operation. An investigation carried out in six New York hospitals found that 43 percent of all uterus operations were unjustified. Fifteen percent of hysterectomies are carried out to remove cancerous tumors, and are thus considered necessary. The other 85 percent are due to uterine fibroids, endometriosis, or other causes of pelvic pain and excessive bleeding. Thousands of women every year have a full hysterectomy (including the removal of the ovaries), but have not given their consent prior to the surgery. First, there is the less invasive nryomectomy, which preserves fertility by removing just the fibroid, but keeps the rest of the reproductive system intact. Of course, there are also a number of natural methods, like the ones explained in this book, that can be used to prevent and remove fibroids and other reproductive disorders. Balancing estrogen levels through liver cleansing and dietary changes is very important for any woman suffering from female disorders. It is a well-known fact that fibroids tend to shrink and disappear after menopause when estrogen levels decrease. The liver is in charge of breaking down estrogen, but is prevented from doing so properly when it is congested with intrahepatic gallstones. Most fibroids develop when congestion of the cisterna chyli vessels (a group of sac-like lymph vessels located in the middle of the abdomen) prevents the proper drainage of metabolic waste products and dead, turned-over cells from the female reproductive organs. By addressing the underlying causes of fibroids, the reproductive organs can resume their full functions. The mortality rate is 1 in 1, 000 procedures, and serious complications occur 15 times more frequently than that. Side effects can occur in more than 40 percent of operations; they include urinary retention or incontinence, significant reduction in sexual response, early ovarian failure, risk of a fatal blood clot and bowel problems. Induction, Cutting and Caesarean Section Pregnant women are generally treated with respect and special care, but the methods of delivery used today can have an adverse effect on mother and baby alike. Before the era of hospital deliveries, the responsibility for handling deliveries was given to competent women. Provided that the appropriate hygienic measures were taken, very few birth complications occurred. Today, however, with most deliveries being handled by male doctors and taking place in the sterile environment of a hospital room, we have the highest rates of complications at birth. Research from Britain, Switzerland and Holland, published by the British Medical Journal in 1996, found that planned home births were the safest of all options, including hospital deliveries. In hospitals, delivering mothers are watched over by a number of electronic instruments and machines that monitor every possible change and that signal the need for an operation just in case something goes wrong. Yet if the mother were not induced and/or made numb by drugs and were properly prepared for the delivery, she would know perfectly well how and when and when not to push to release the child from the birth canal at the right time. Even if it did tear, the injury would heal much faster than a cut inflicted by a surgical knife. The second most unnecessary but most commonly applied operation during delivery is the Caesarean section.
Cheap grisactin 250 mg
The next few figures illustrate some of the common normal and abnormal bulges we encounter in daily practice treatment pancreatitis buy cheap grisactin. Red arrows point to a bulge in the right superior mediastinum, which proved to be a bronchogenic carcinoma after an angiogram eliminated the possibility of a vascular shadow. The vertical stripes over the right side of the chest are computer or scanner artifacts. Yellow arrow points to another bulge along the right superior mediastinum, but this time representing a normal finding, a prominent azygous vein. Blue arrows point to abnormal bulges of the mediastinum, which proved to be benign teratomas. Blue arrows point to full, abnormal hilar shadows, which proved to be hilar adenopathy in a patient with lymphoma. Red arrows point to abnormal mediastinal contour, which proved to be another lymphomatous mass. The aorta is filled with iodinated contrast, which accounts for its bright white appearance. Note the encroachment on the arch of the aorta, which accounts for the positive silhouette sign. For example the figures below show mediastinal densities not seen on a normal radiograph of the chest. The gas in this case represents gas in the fundus of the stomach and is thus diagnostic of a hiatus hernia. The lateral view of the patient in figure #46 shows the gas bubble in the herniated stomach above the diaphragm (small arrows). The lateral view also shows an air fluid level in the stomach (red arrow) confirming the diagnosis of hiatal hernia. The red arrow points to gas in the fundus of the stomach, which you saw on the chest radiograph. Red outlined arrow points to a relatively horizontal left mainstem bronchus, which is elevated by an enlarged left atrium, secondary to mitral valvular stenosis. Note that it does not silhouette out the left heart border or left pulmonary artery. The red outlined arrows point to the posterior margin of a descending thoracic aortic aneurysm. Red arrow points to another double density in the mediastinum, this time representing gas density, but not in a location for hiatus hernia. Barium in the esophagus demonstrates a large diverticulum (red arrows) containing a bezoar (yellow arrow) and air (blue arrow) which accounts for the double density seen on the plain film radiograph. Also note a calcified granuloma (green arrows) which was present in figure 54 but not well demonstrated in the underpenetrated film. This is where the value of the lateral projection comes in handy to explain any double densities or shadows you are worried about. The silhouette sign is extremely important in assessing for fluid or pleural thickening, and in order to tell the difference a lateral decubitus view will answer the question of free fluid, especially if no prior films are available for comparison. There is also a variant of the diaphragm with which you should become familiar which is an eventration, simply a weakness of the muscle fibers of the diaphragm usually congenital in origin, and which can effect either leaf. Eventrations cause the hemidiaphragm to appear elevated, but usually are of no clinical significance or importance in asymptomatic adults. Eventrations in the newborn may cause respiratory distress in some cases and are subject to surgical intervention. Images in figures 56 and 57 courtesy of Madigan Army Medical Center via the Internet. A Bochdalek hernia, demonstrated below, is the most common of the diaphragmatic hernias and the most common surgical emergency of the neonate when it compromises lung capacity. White contrast in distal stomach Pink herniated stomach Orange-spleen Red aorta Yellow kidneys Blue rt. Red arrows point to diaphragmatic calcifications in this patient with documented asbestos exposure. The last major system to evaluate in the chest radiograph aside from a couple of other tips is the bony thorax. I tell my students that after looking at chest radiographs for 30 years I can usually see everything at once but that it took years of practice and looking at every bone before I felt comfortable with it. I still carefully examine every bone, (now using a magnifying glass) if looking for fractures or metastatic pathology. I further inform them that to reach a level of competence, the practice of scrutinizing each bone is an absolute necessity, and that to program that computer between their ears to easily spot abnormalities of the bony thorax can not be done in a short period of time. Just to illustrate the point, see if you can spot the bony abnormalities in the following figures before reading the answers under each picture. See if you can spot any bony abnormalities (subtle) before referring to the sketch below. The negative study of an aortic arch angiogram in this same patient shows the coarctation (white arrow) in Figure # 63b (below). The next case (below) demonstrates another bony abnormality that may be difficult to see for the inexperienced eye. Tomograms of this area shown in figures 66 and 67 on the next page demonstrate the bone destruction caused by metastatic carcinoma. This sounds like a lot to consider, but in actuality the student will quickly make a decision as to whether or not the pattern is normal. If it is not, one then has to decide why not, and also if the pattern is specific or non-specific. The chest film is included for two reasons: 1) Many chest conditions such as pneumonia or pleural effusions can present as abdominal pain and 2) It gives us a chance to look at the diaphragm and for free air. The upright or decubitus view lets us look for localizing signs such as air fluid levels or isolated and dilated loops of bowel. Sometimes we are only given a single view to interpret, especially when the film comes from an outside source (St. If one observes gas filled, dilated loops of bowel, we must then decide whether or not we are dealing with an adynamic ileus, an obstructive ileus, a localizing phenomenon such as might occur with appendicitis, cholecystitis or pancreatitis (sentinel loop), or a natural finding as occurs with aerophagia in a crying child or air forced into the gut during general anesthesia. It is also important to recognize whether or not the gas is in large or small bowel. That is not always possible, but one of the things that helps tell the difference is to see if the haustral markings extend all the way across the loop or only part way. Colon haustral markings typically traverse only part of the way across the loop, whereas small bowel haustra usually extend the full diameter of the loop. Obstructive ileus is usually oriented in an up and down or vertical pattern, whereas paralytic ileus is usually oriented in a transverse plane. Yellow arrows point to multiple air-fluid levels in this patient with obstructive ileus, the red curved arrows show the haustral markings extend the entire diameter of the bowel, thus identifying it as small intestine. Note there is very little gas in the colon, that the small bowel is markedly dilated and that these loops are vertically oriented. Red arrows point to haustra that do not traverse the diameter of the bowel indicating the dilated loops of this portion are likely colon. Note that both small and large bowel are dilated and that the loops have a relatively horizontal 54 orientation. This patient has a paralytic or non-obstructive ileus, with gas extending all the way to the rectum. Localization of gas in the intestine in a dilated segment or region occurs with a confined inflammatory process such as appendicitis (right lower quadrant), cholecystitis (right upper quadrant) or pancreatitis (sentinel loop). Gas may also appear in bile ducts or other extra-luminal locations under certain conditions. These radiographic findings are not specific, but do tend to localize an inflammatory process, and appendicitis should be included in the differential diagnosis. The next figure (#71) is a coned-down view of the right lower quadrant in this same patient.
250mg grisactin for sale
Treat for (ext racellular or with abnormal morphology) gonorrhea and Chlamydia infect ions medicine 2000 purchase cheap grisactin on line. Patients who have frequent outbreaks may be candidates for Patients with secondary syphilis can also have a chronic acyclovir suppression. Syphilis is characterized by stages of active clinical disease separated by periods of asymptomatic latent infection. Factors that could lead toward inpatient tions that can produce symptoms suggestive of a. If examination of a cover-slipped slide antibiotic therapy for an isolated organism may be of unspun urine under 40x power reveals one efective, hut reinfection with diferent organisms is organism per feld (Figure 30-1), this correlates common. Urinalysis (dipstick and/or microscopic) and with recurrent infections with Prteus), and the culture are the most important laboratory tests. A number of factors (see "Risk systems, pulmonary tuberculosis remains the most Factors") have led to this increase, including the important manifestation. In most cases the initial infection is walled off by granuloma formation, but viable organisms may History persist within the granuloma. When malignancy, or corticosteroid administration), these symptoms do develop later in the disease, they are organisms may escape from the granuloma resulting, usually nonspecifc and constitutional: in reactivation tuberculosis. Acid-fast positivity requires a heavy organism burden in the patient, and Development of hemoptysis denotes advanced early disease may be missed. It is important to phylaxis in patients with a positive skin test of note that in 33 states (representing approximately unknown duration. Gastroenteritis is also frequently encountered in the international Bacteria, viruses, and protozoans can cJuse acute traveler. The most commonly encountered viral pathogens are caliciviruses, rotavirus, and the parvoviruses. Ingestion of contaminated food or controlled, causing a short-lived (24 to 48-hour) drink is generally most common, but swimming or illness. Entamoeba histolytica dling practices are not commonly observed is often and Giardia Lamblia are two of the most commonly associated with development of gastroenteritis, but encountered protozoan pathogens. The former lapses in food handling also occur in the home and invades the colon, causing a bloody diarrhea, whereas in restaurants under a number of circumstances: Giardia colonizes the small intestine, causing a malabsorptive syndrome and an osmotic diarrhea. A history of the presence of stool leukoytes generally suggests known infection with human immunodeficiency a bacterial pathogen. If a protozoan etiology is suspected, examination Ingestion of preformed toxin. Infection with a pathogenic but in some cases this is inconvenient and special bacterium that needs to replicate to cause disease containers with stool preservatives can be used. In the majority of cases, the the severity of the illness can be indicated by condition will resolve on its own with symptomatic signs of dehydration such as orthostatic hypotension, therapy. Certain infections require administration of dry mucosal membranes, and decreased skin antimicrobials for clearance (see below and Table turgor. Invasion of colon Fever, bloody diarrhea with Antibiotics fecal leukocytes; fecalforal spread Vibrio cholere Enterotoxin Profuse watery diarrhea; fever Doxycycline is rare; fecal/oral spread (often via water contamination) < not for sale! Concerns solutions that contain electrolytes and glucose should about routine antibiotic use include the widespread be used. For this reason, many experts recommend difficult, administration of intravenous fluids may treatment of documented Salmonella infections become necessary. Recent evidence shows that atropine-containing compounds (Lomotil) can be treatment of E. Fresh fruits should be peeled by the form to stools but do not decrease the fluid content consumer just prior to consumption. These cardiac abnormalities), circulating bacteria, and the are caused either by microemboli or macroemboli or host immune system.